- Visibility 17 Views
- Downloads 13 Downloads
- DOI 10.18231/j.ijooo.2024.028
-
CrossMark

A deep dive into penetrating ocular trauma: Insights from a South Indian tertiary eye care center
Introduction
Ocular trauma is a preventable public health issue that is the leading cause of blindness in children, ophthalmic morbidity, and monocular blindness worldwide.[1] One in every twenty patients who visits an ophthalmologist has an eye injury.[2]
Ocular injury etiologies vary across nations, regions of the world, and demographic or socio-economic strata. Early detection and intervention are the key to trauma management and prevention of further complications.[3], [4], [5] Whether the trauma is minor or severe, in an urban or rural setting, or involving an adult or child, the patient must be medically stabilized and the eye thoroughly assessed.[6]
Penetrating ocular trauma remains a significant cause of visual impairment and blindness worldwide. In South India, where industrial and agricultural activities are prevalent, the incidence of ocular trauma is notably high. This study aims to provide a comprehensive overview of the clinical profile of penetrating ocular trauma at a tertiary eye care center in South India, focusing on demographic patterns, causes, management, and outcomes.
Materials and Methods
A retrospective study was conducted on patients with penetrating ocular trauma treated at a tertiary eye care center in South India from January 2024 to June 2024. Data were extracted from medical records, including demographic information, mode of injury, clinical presentation, surgical interventions, and visual outcomes. Statistical analyses were performed to identify patterns and correlations.
Results
Demographic characteristics
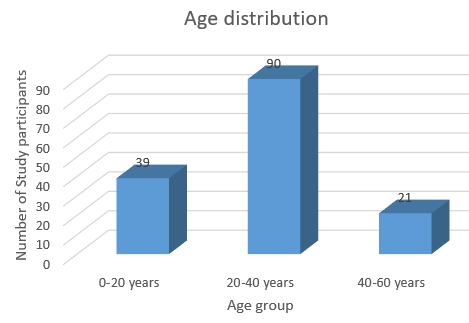
A total of 150 patients were included, with a male predominance (80%). The age distribution showed a peak incidence in the 20-40 age group (60%). ([Figure 1])
The mean age at presentation was 28 years.
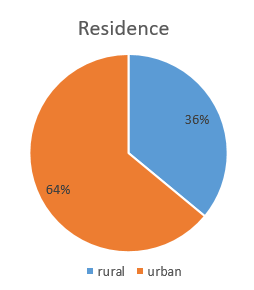
There was significant difference between rural (64 %) and urban (36%) population. ([Figure 2])
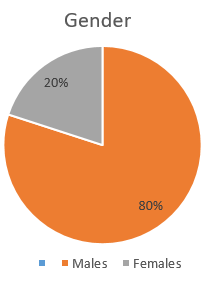
There were 120 (80%) males and 30 (20%) females. ([Figure 3])
Causes of trauma
Workplace injuries were the leading cause (45%), followed by domestic injuries (30%) and road traffic accidents (10%). Other causes included sports injuries and assaults.([Table 1])
|
S.No. |
Type of injury |
Number of study of participants |
Percentage |
|
1. |
Workplace injuries |
68 |
45% |
|
2. |
Domestic injuries |
45 |
30% |
|
3. |
Road traffic accidents |
22 |
15% |
|
4. |
Sports injuries and assaults |
15 |
10% |
Ocular injury details
One hundred forty four study participants (96%) had uniocular and 6 study participants (4%) had binocular injuries.
Of the participants who sustained uniocular injury, Left eye was involved in 76 participants (53%) and Right eye in 68 participants (47%).([Table 2])
|
Laterality |
Number of study participants |
|
Right eye |
68 |
|
Left eye |
76 |
|
Both eyes |
06 |
[Figure 4], [Figure 5] depict some injuries due to penetrating trauma.


Mode of injury
Injury with metal fragments were the most common inciting factor for penetrating injury, accounting to 42 cases (28%), followed by injury with wooden splinters, glass pieces, scissors/needles, projectile, sickle/knife and road traffic accidents.([Table 3])
|
Mode of injury |
Count (n=150) |
Percentage |
|
Metal fragments |
42 |
28% |
|
Wooden splinters |
29 |
19% |
|
Glass piece |
12 |
8% |
|
Scissors/needle |
18 |
12% |
|
Projectile (stone/stick) |
17 |
11% |
|
Sickle |
8 |
5% |
|
Knife |
9 |
7% |
|
Road traffic accidents |
15 |
10% |
Clinical presentation
Initial visual acuity at presentation ranged from no light perception to >6/18. Most patients (36%) had an initial visual acuity between 5/60 and CF@CF. Common symptoms included pain, redness, and vision loss.([Table 4])
|
S.No. |
Vision at presentation |
Number of study participants |
|
1. |
>6/18 |
11 |
|
2. |
6/18 – 6/60 |
19 |
|
3. |
5/60 – CF@CF |
54 |
|
4. |
HM – PL |
40 |
|
5. |
NPL |
26 |
Clinical findings
Most patients presented with a corneal tear (32%), followed by corneoscleral tear (29%), scleral tear (23%) and corneolimbal tear (16%). These patients also had associated findings like traumatic cataract, vitreous hemorrhage, vitreous loss, hyphema, uveal prolapse and retinal detachment.([Table 5])
|
Type of injury |
Number of study participants |
|
Corneal tear |
48 |
|
Corneoscleral tear |
44 |
|
Corneolimbal tear |
24 |
|
Scleral tear |
34 |
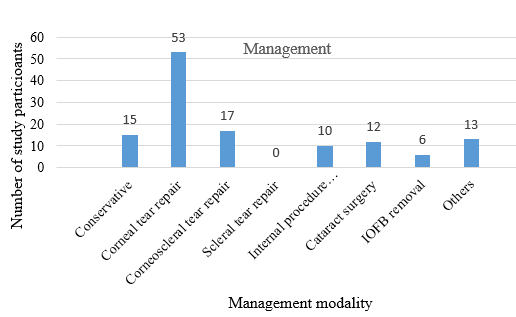
Management
90% of patients (n=135) required surgical intervention, including repair of the corneal/scleral laceration, IOFB removal and vitrectomy. Post-operative care included systemic and topical antibiotics, anti-inflammatory medications, cycloplegics and follow-up visits.([Figure 6])
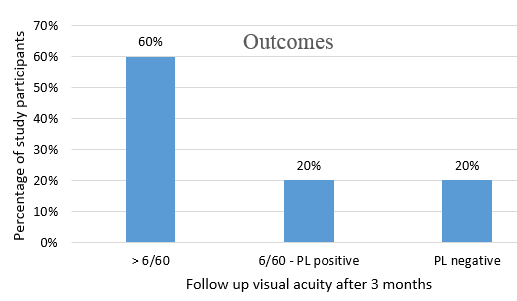
Outcomes
At the follow-up after 3 months, 60% of patients achieved a visual acuity of 6/60 or better. 20% had no light perception, and the remainder had varying degrees of visual impairment. Factors influencing outcomes included the severity of the injury, time to surgery, and presence of intraocular foreign bodies.([Figure 7])
Discussion
Penetrating ocular injuries represent a significant challenge in ophthalmic care, particularly in regions with varying socioeconomic conditions and access to healthcare. This study provides a comprehensive analysis of the clinical profile of penetrating ocular trauma at a tertiary care center in South india, shedding light on patterns, outcomes, and implications for future management.
In this study, most ocular traumas occurred between 20 and 40 years because people in their second to fourth decade of life are more active and thus more vulnerable to ocular trauma. Males 80% (n=120) were more likely to sustain traumatic injuries than females due to more males involved in driving, industrial and agricultural occupations.
The predominance of rural patients highlights disparities in access to preventive eye care and immediate medical attention, suggesting that targeted education and improved safety measures in these areas could mitigate the risk of such injuries.
In our study 60% of cases presented to casualty within six hours of injury. Only 10% of cases presented after 24 hours. Patients presenting early and promptly in this region may signify better awareness of ocular trauma in the population as our hospital is the primary referral center.
According to the JUDO study, the cornea was the most affected part of the eye (63.2%) in any ocular trauma, which was also confirmed in Menelik II Hospital studies. [7], [8] Our study also showed an involvement of cornea in 66% of the cases.
The primary causes of penetrating ocular injuries in our study were workplace accidents (45%), domestic injuries (30%), and road traffic accidents (15%). This distribution mirrors patterns observed in other developing countries, underscoring the need for specific preventive strategies tailored to these common injury sources. Additionally, the high proportion of injuries related to agricultural activites points to the necessity for better protective measures and training for those involved in such high risk enviroments.
The clinical presentation of penetrating ocular injuries varied widely, with corneal and scleral lacerations being the most common types. The variability in clinical outcomes also emphasizes the importance of timely intervention and the role of initial injury severity in predicting visual prognosis.
The study underscore the need for targeted public health interventions, including educational programs on eye safety and the implementation of preventive strategies, particularly in high risk populations. [9] Enhanced training for healthcare providers in managing ocular trauma and increasing awareness about the importance of early treatment can contribute to better outcomes.
The management of penetrating ocular injuries in South India is hindered by several factors, including delayed presentation, limited access to specialized care, and the cost of treatment. [10] Addressing these challenges requires a multi-faceted approach, involving improved awareness, enhanced access to healthcare, and targeted prevention strategies.
Future research is essential to further elucidate the epidemiology, clinical profile, and management of POIs in South India. This will enable the development of more effective prevention and treatment strategies to reduce the burden of visual impairment associated with these injuries. [11] By addressing the underlying causes and improving access to care, it is possible to mitigate the devastating consequences of penetrating ocular injuries on the lives of individuals and communities in South India. [12]
Conclusion
Penetrating ocular trauma in South India is predominantly associated with industrial and domestic accidents. Effective management, including timely surgical intervention, can improve visual outcomes. Enhanced public education and preventive strategies are essential to reduce the incidence of such injuries. Visual prognosis can be effectively explained to the patient with regular use of ocular trauma score. [13], [14]
This study provides a comprehensive analysis of the clinical profile of penetrating ocular trauma in South India, highlighting significant patterns and implications for healthcare practice in the region. The findings reveal that penetrating ocular trauma is a major public health concern, with a high incidence of injuries resulting from workplace accidents, domestic injuries and road traffic accidents. The demographic analysis indicates a predominance of injuries among males, particularly in younger age groups, emphasizing the need for targeted preventive measures in high-risk populations. [15] The clinical presentation of penetrating ocular trauma in this region is characterized by a variety of injury types, including corneal and scleral lacerations, vitreous hemorrhage, and traumatic cataract. [16] The majority of patients present with severe visual impairment, underscoring the critical need for timely and effective management.
In summary, addressing penetrating ocular trauma in South India requires a multifaceted approach that includes improving access to timely medical care, implementing preventive measures, and investing in healthcare infrastructure. Continued research and collaborative efforts between healthcare providers, policymakers, and community organizations are essential to reduce the incidence and impact of ocular trauma and to enhance patient outcomes in the region.
Source of Funding
None.
Conflict of Interest
None.
References
- R Dagwar, S Jawade, R Chauhan. Clinical Profile and Visual Outcome of Blunt Ocular Trauma in a Tertiary Care Centre of Central India: A Prospective Study. Int J Med Sci Clin Invention 2020. [Google Scholar] [Crossref]
- L Mowatt, A Mcdonald, D Ferron-Boothe. Hospitalization trends in adult ocular trauma at the University Hospital of the West Indies. West Indian Med J 2012. [Google Scholar]
- S Nadeem, M Ayub, H Fawad. Visual Outcome of Ocular Trauma. Pak J Ophthalmol 2013. [Google Scholar]
- F Kuhn, R Morris, C D Witherspoon. Birmingham Eye Trauma Terminology (BETT): terminology and classification of mechanical eye injuries. Ophthalmol Clin North Am 2002. [Google Scholar]
- . Ocular trauma during COVID- 19 crisis: Trends and management. RP Maurya 2020. [Google Scholar]
- SC Kaufman, DR Lazzaro. . Textbook of Ocular Trauma 2017. [Google Scholar]
- KD Alem, DD Arega, ST Weldegiorgis, BG Agaje, EG Tigneh. Profile of ocular trauma in patients presenting to the department of ophthalmology at Hawassa University: Retrospective study. PLoS One 2019. [Google Scholar] [Crossref]
- T Asaminew, Y Gelaw, F Alemseged. A 2-year review of ocular trauma in Jimma University Specialized Hospital. Ethiop J Health Sci 2009. [Google Scholar]
- AW Scott, NM Bressler, S Ffolkes, JS Wittenborn, J Jorkasky. Public attitudes about eye and vision health. JAMA Ophthalmol 2016. [Google Scholar]
- E Syal, M Dhawan, SP Singh. To study the epidemiological and clinical profile of ocular trauma at a tertiary health-care facility. Delta J Ophthalmol 2018. [Google Scholar] [Crossref]
- AD Négrel, B Thylefors. The global impact of eye injuries. Ophthalmic Epidemiol 1998. [Google Scholar]
- ED Kyriakaki, EK Symvoulakis, G Chlouverakis, ET Detorakis. Causes, occupational risk and socio-economic determinants of eye injuries: a literature review. Med Pharm Rep 2021. [Google Scholar]
- F Kuhn, R Maisiak, L Mann, V Mester, R Morris, C D Witherspoon. . Ophthalmol Clin North Ama 2002. [Google Scholar]
- MA Shah, SM Shah, A Applewar, C Patel, S Shah, U Patel. Ocular Trauma Score: a useful predictor of visual outcome at six weeks in patients with traumatic cataract. Ophthalmology 2012. [Google Scholar]
- B M Zagelbaum, J R Tostanoski, D J Kerner, P S Hersh. Urban eye trauma: a one-year prospective study. Ophthalmology 1993. [Google Scholar]
- R Agrawal, G Rao, R Naigaonkar, X Ou, S Desai. Prognostic factors for vision outcome after surgical repair of open globe injuries. Indian J Ophthalmol 2011. [Google Scholar]