- Visibility 514 Views
- Downloads 57 Downloads
- Permissions
- DOI 10.18231/j.ijooo.2024.025
-
CrossMark

Eye on impact: An analysis of blunt ocular trauma cases at a tertiary eye care centre in South India
Abstract
Aims: This study investigates the epidemiology, injury mechanisms, and clinical features of blunt ocular trauma. It aims to assess the prevalence of these injuries and the extent of vision loss among patients at a tertiary eye care center in South India.
Materials and Methods: A retrospective observational study was conducted at a teaching hospital over four months, from June 2024 to September 2024. The study included 417 patients of all age groups who visited the outpatient department of a tertiary eye care center after experiencing blunt ocular trauma. Data were collected on the cause and circumstances of the injury, injury mechanism, clinical features, management, and visual outcomes.
Results: This study included 417 patients, with the majority falling into the 21–30 year age group. Men had a higher rate of eye injuries than women, and the most common cause of injury was road traffic accidents (35.97%). The predominant type of ocular injury was closed globe injuries, with an incidence of 95.92%. Additionally, 17.2% of the patients required surgical intervention.
Conclusion: Most blunt ocular trauma is caused by road traffic accidents, followed by physical assaults, with young men being the most affected. This underscores the need for preventive measures, such as wearing helmets and avoiding driving under the influence of alcohol, to reduce the incidence of these injuries. Public awareness campaigns can play a vital role in promoting safety and protecting vulnerable populations.
Introduction
Blunt ocular trauma is one of the most common eye injuries, particularly in younger individuals, and blunt objects account for approximately 30% of all such injuries. The primary cause is road traffic accidents, followed closely by occupational hazards.[1]
Blunt ocular trauma can result in either open or closed globe injuries. Closed globe injuries, where the outer structure of the eye remains intact, are classified into contusions, caused by blunt impact, and lamellar lacerations, which involve partial-thickness cuts. Open globe injuries, where the outer eye is breached, are categorized into lacerations, caused by sharp objects, and globe ruptures, which occur when the eye is severely damaged by blunt force. [2]
Blunt ocular trauma can result from coup and countercoup forces, as well as anteroposterior compression or horizontal tissue expansion. [3] Coup injuries occur at the site of impact, resulting in conditions such as subconjunctival hemorrhage, corneal abrasions, and subretinal or choroidal hemorrhages. Contrecoup injuries, on the other hand, occur on the opposite side of the impact due to shock waves passing through the eye, as seen in conditions like commotio retinae. [4]
Blunt ocular trauma can result in a broad spectrum of complications, ranging from minor injuries, such as subconjunctival hemorrhage, to severe, vision-threatening conditions like optic neuropathy, retinal detachment, and traumatic cataracts.
Materials and Methods
All cases of blunt eye injuries that sought care at the outpatient department of a tertiary eye care hospital from June 2024 to September 2024 were collected and analyzed from the medical records archive. A total of 417 patients were included in the study. Exclusion criteria comprised ocular injuries resulting from penetrating injuries, perforating injuries, chemical injuries, and thermal injuries. Data collected included demographic details, the mode of injury, and clinical presentation. Orbital imaging was obtained in cases with suspected orbital wall fractures. The ocular injuries were classified into open and closed globe injuries using the Birmingham Eye Trauma Terminology System. [5] The results were analyzed and presented in tabular form.
Results
Demographic characteristics
|
Demographic variable |
|
Numbers (N=417) |
Percentage |
|
Age group |
<1 year |
2 |
0.47% |
|
1-10 years |
41 |
9.83% |
|
|
11 – 20 years |
96 |
23.02% |
|
|
21 – 30 years |
101 |
24.22% |
|
|
31 – 40 years |
70 |
16.78% |
|
|
41 – 50 years |
57 |
13.66% |
|
|
51 – 60 years |
28 |
6.71% |
|
|
61 – 70 years |
15 |
3.59% |
|
|
71 – 80 years |
5 |
1.19% |
|
|
81 – 90 years |
2 |
0.47% |
|
|
91 -100 years |
0 |
0 |
|
|
Sex |
Male |
338 |
81.05% |
|
Female |
79 |
18.94% |
|
|
Household |
Urban |
303 |
72.66% |
|
Rural |
114 |
27.33% |
The study included 417 patients with blunt trauma injuries, ranging in age from newborns to 100 years, with an average age of 30. This suggests that the majority of the patients were in the young, productive age group ([Table 1]).
Eye injuries were notably more common in males, who accounted for 81% of cases ([Table 1]).
In our study, a higher proportion of patients came from urban households, with an incidence rate of 73%, compared to rural areas ([Table 1]).
Circumstances of injury
|
|
|
Numbers (N =417) |
Percentage |
|
Place of injury |
Road/Street |
272 |
65.22% |
|
Home |
94 |
22.54% |
|
|
Workplace |
25 |
5.99% |
|
|
|
Playground |
26 |
6.23% |
The majority of injuries occurred on the road or street (65.22%), followed by those that took place at home (22.54%) ([Table 2]).
|
|
|
Numbers (N =417) |
Percentage |
|
Modes of injury |
Road traffic accident |
150 |
35.97% |
|
Assault |
107 |
25.65% |
|
|
Workplace |
25 |
5.99% |
|
|
Self fall |
41 |
9.83% |
|
|
Sports related |
26 |
6.23% |
|
|
Miscellaneous |
68 |
16.30% |
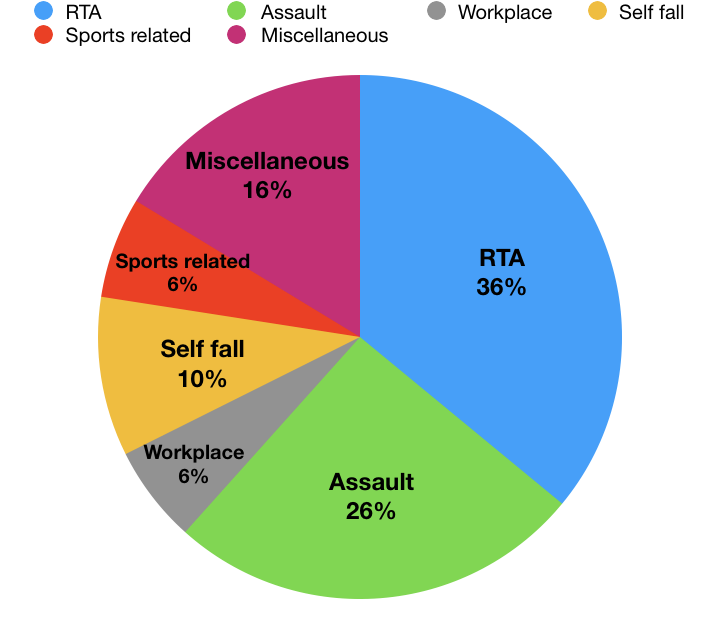
Among the 417 cases of blunt ocular trauma, road traffic accidents were the most common cause (35.97%), followed by assaults (25.65%) ([Table 3]).
|
|
|
Numbers (N= 136) |
Percentage |
|
Agents of blunt ocular trauma |
Hand |
106 |
77.94% |
|
Wood |
41 |
30.14% |
|
|
Metal |
22 |
16.17% |
|
|
Stone |
16 |
11.76% |
|
|
Plastic |
12 |
8.82% |
|
|
Cricket ball |
21 |
16.17% |
|
|
Shuttlecock |
4 |
2.94% |
|
|
Snooker stick |
1 |
0.73% |
|
|
Bull horn |
3 |
2.20% |
The most frequent agent of trauma was the hand (77.94%), followed by wood (30.14%) ([Table 4]).
Time of presentation
|
|
|
Numbers (N =417) |
Percentage |
|
Time of presentation |
With in 1 day |
395 |
94.72% |
|
After week |
5 |
1.19% |
|
|
After 1 month |
5 |
1.19% |
|
|
After 1 year |
8 |
1.91% |
|
|
After 2 year |
2 |
0.47% |
|
|
After 20 year |
2 |
0.47% |
The majority (94.72%) of cases of blunt ocular trauma presented on the same day as the injury ([Table 5]). Out of the 417 cases, 285 were medico-legal cases (MLCs).
Pattern of injury
|
Characteristics |
|
Numbers (N =417) |
Percentage |
|
Laterality |
Right eye |
188 |
45.08% |
|
Left eye |
189 |
45.32% |
|
|
Bilateral |
49 |
11.75% |
|
|
Type of injury |
Open globe |
17 |
4.07% |
|
Closed globe |
817 |
95.92% |
Out of 417 blunt trauma cases, 45.32% involved the left eye, 45.08% involved the right eye, and 11.75% affected both eyes. Additionally, 17 patients (4.07%) had open globe injuries ([Table 6]).
Presentation
|
Ocular structure involved |
Numbers (N=977 ocular structure) |
Percentage |
|
Orbit |
36 |
3.68% |
|
Extraocular muscle |
12 |
1.22% |
|
Adenexa |
458 |
46.87% |
|
Globe |
16 |
1.63% |
|
Conjunctiva |
165 |
16.88% |
|
Sclera |
17 |
1.74% |
|
Cornea |
31 |
3.17% |
|
Anterior chamber |
42 |
4.29% |
|
Iris and pupil |
37 |
3.78% |
|
Lens and IOL |
18 |
1.84% |
|
Vitreous |
19 |
1.94% |
|
Retina |
78 |
7.98% |
|
Optic Nerve |
48 |
4.91% |
Out of 977 eye structures affected by blunt trauma, the most commonly involved was the adnexa (46.87%), followed by the conjunctiva (16.88%) ([Table 7]).
|
Characteristics |
|
Numbers (N=834 eyes) |
Percentage |
|
Presenting Visual acuity |
6/6 – 6/12 |
624 |
74.82% |
|
6/18 – 6/60 |
58 |
6.95% |
|
|
CF@3m – HM+ve |
95 |
11.39% |
|
|
PL positive |
24 |
2.87% |
|
|
PL negetive |
25 |
2.99% |
|
|
Couldn’t be assessed |
8 |
0.95% |
|
|
Orbital |
Floor fracture |
16 |
1.91% |
|
Medial wall fracture |
7 |
0.83% |
|
|
Lateral wall fracture |
9 |
1.07% |
|
|
Roof fracture |
1 |
0.11% |
|
|
Retrobulbar haemorrhage |
3 |
0.35% |
|
|
Muscle movement restriction and limitation |
Inferior rectus entrapment |
2 |
0.23% |
|
Oculomotor palsy |
5 |
0.59% |
|
|
Abducens palsy |
5 |
0.59% |
|
|
Adenexa |
Periorbital edema |
208 |
24.94% |
|
Ecchymosis |
160 |
19.18% |
|
|
Lid laceration |
57 |
6.83% |
|
|
Lid abrasion |
6 |
0.71% |
|
|
Lid hematoma |
4 |
0.47% |
|
|
Preseptal cellulitis |
5 |
0.59% |
|
|
Brow laceration |
6 |
0.71% |
|
|
Mechanical Ptosis |
7 |
0.83% |
|
|
Canalicular tear |
5 |
0.59% |
|
|
Globe |
Proptosis |
7 |
0.83% |
|
Enophthalmous |
5 |
0.59% |
|
|
Pthysis bulbi |
4 |
0.47% |
|
|
Conjunctiva |
Conjunctival laceration |
11 |
1.31% |
|
Chemosis |
5 |
0.59% |
|
|
Subconjunctival haemorrhage |
149 |
17.86% |
|
|
Sclera |
Globe rupture |
13 |
1.55% |
|
Sclerocorneal tear |
4 |
0.47% |
|
|
Cornea |
Corneal abrasion |
2 |
0.23% |
|
Corneal tear |
28 |
3.35% |
|
|
Wound dehiscence of TPK |
1 |
0.11% |
|
|
Anterior chamber |
Hyphema |
16 |
1.91% |
|
Uveitis |
26 |
3.11% |
|
|
Iris and pupil |
Iris prolapse |
12 |
1.43% |
|
Iridodonesis |
1 |
0.11% |
|
|
Iridodialysis |
6 |
17.64% |
|
|
Traumatic mydriasis |
18 |
2.15% |
|
|
Lens and IOL |
Traumatic cataract |
3 |
0.35% |
|
Phacodonesis |
1 |
0.11% |
|
|
Subluxated lens |
10 |
1.19% |
|
|
Subluxated IOL |
4 |
0.47% |
|
|
Vitreous |
Vitreous Haemorrhage |
19 |
2.27% |
|
Retina |
Retinal haemorrhage |
5 |
0.59% |
|
Berlin edema |
32 |
3.83% 1.43% |
|
|
Commotio retina |
12 |
||
|
Macular hole |
4 |
0.47% |
|
|
Retinal detachment |
25 |
2.99% |
|
|
Optic nerve |
Traumatic optic neuropathy |
48 |
5.75% |
In 74.82% of patients, vision was better than 6/12, while 2.99% presented with no perception of light. Periorbital edema was the most common finding, occurring in 24.94% of cases ([Table 8]).

Mangement
Surgical procedures were performed on 17.2% of the affected eyes, including both minor outpatient operations and major surgeries that required hospitalization.
Discussion
Blunt objects are the most common cause of mechanical ocular trauma. In this study, it was observed that the majority of injuries (24.22%) occur among productive young people aged 21 to 30 years, with males (81%) more commonly sustaining blunt ocular trauma compared to females (19%). This aligns with the findings of Nayagam et al.[6] This male predominance appears to be linked to outdoor activities, engagement in hazardous recreational activities and sports, risk-taking behaviors, alcohol consumption, and personal conflicts.
The present study revealed a higher prevalence of blunt ocular trauma in the urban population (73%) compared to the rural population (27%), consistent with the findings of Sujatha et al.[7] who reported that 78% of blunt trauma occurred in the urban population.
In the current study, the most common place of injury was the street or road (65.22%), followed by the home (22.54%), workplace (5.99%), and playground (6.23%). This is consistent with the findings of the study by Maurya et al.[8]
In this study, the most common cause of blunt ocular trauma was road traffic accidents (35.97%), which aligns with the findings of Pai et al.[9]
The majority of ocular blunt trauma cases (94.72%) were presented on the same day as the injury, while 5.28% of cases were presented late, more than a week after the incident. This is consistent with the findings of Mishra et al.[10]
The most frequent cause of trauma was the hand (77.94%), followed by wood (30.14%). In contrast, wood was identified as the most common agent in the study conducted by Maurya et al.,[6] while metallic objects were the most common in the study by Syal et al.[11]
The majority of victims (90.4%) experienced unilateral blunt ocular trauma, with a predominance of left eye involvement (45.32%). In contrast, only 11.75% had bilateral involvement, which aligns with the findings of Maurya et al.[12], [13]
Most injuries were closed globe injuries (95.93%), while 4.07% were open globe injuries. This is consistent with the study by Marudhamuthu et al.,[14] which reported a closed globe injury rate of 95.3%.
The most commonly affected ocular structure was the adnexa (46.87%), followed by the conjunctiva (16.88%). Periorbital edema was the most frequent finding, observed in 24.94% of cases.
Conclusion
Ocular trauma is a significant cause of avoidable, primarily monocular visual morbidity (visual impairment and blindness), with more than half of blinding injuries now occurring at home.[15] Our study concludes that blunt trauma is the most common ocular injury, primarily caused by road traffic accidents, physical assaults, and sports-related injuries, with young adult males being the most vulnerable. Road traffic accidents are mainly due to skids and falls. Sports-related injuries are more prevalent among children and young adults.[16]
Source of Funding
None.
Conflict of Interest
None
References
- Kumar J, Tolia S. Ocular Blunt Trauma In Bundelkhand Region: A Retrospective Study In Bundelkhand Region. Int J Adv Res. 2024. [Google Scholar] [Crossref]
- Mutie D, Mwangi N. Assessing an eye injury patient. Community Eye Health. 2015;28(91):46-8. [Google Scholar]
- Maiya A, Dharmesh A, Jayaram R. Clinical profile of ocular blunt trauma in a rural hospital. J Clin Ophthalmol Res. 2018;6(1):3-7. [Google Scholar]
- Wolter J. Coup-contrecoup mechanism of ocular injuries. Am J Ophthalmol. 1963;56:785-96. [Google Scholar] [Crossref]
- Dogramaci M, Erdur S, Senturk F. Standardized Classification of Mechanical Ocular Injuries: Efficacy and Shortfalls. Beyoglu Eye J. 2021;6(3):236-42. [Google Scholar]
- Nayagam G, Raman M, Anuradha A, Sheela S, Chakravarthy N. Assessment of visual prognosis using ocular trauma score in open globe injury at a tertiary care centre. TNOA J Ophthalmic Sci Res. 2020;58(1):9-13. [Google Scholar]
- Sujatha M, Nazlin A, Prakash S, Nousheen S. Prevalence of Visual Impairment after Blunt Ocular Trauma in a Tertiary Hospital. Int J Sci Stud. 2015;3(4):36-9. [Google Scholar]
- Singh A, Maurya R, Singh V, Gautam S, Kumar A, Mishra C. Study of epidemiology, clinical profile, visual outcome and prognostic factors of blunt ocular trauma in a teaching hospital. Indian J Clin Exp Ophthalmol. 2022;8(4):458-67. [Google Scholar]
- Pai S, Karnath SJ, D'Souza S, Dudeja L. A clinical study of blunt trauma in a Tertiary care centre. Online J Health Allied Sci. 2013;12(2). [Google Scholar]
- Mishra A, Verma A, Baranwal V, Aggarwal S, Bhargava N, Parihar J. The pattern and visual outcomes of ocular trauma in a large zonal hospital in a non-operational role A 36 months retrospective analysis. J Clin Ophthalmol Res. 2014;2(3):141-4. [Google Scholar]
- Syal E, Dhawan M, Singh S. To study the epidemiological and clinical profile of ocular trauma at a tertiary health-care facility. Delta J Ophthalmol. 2018;19(4):259-67. [Google Scholar]
- Maurya R, Singh V, Kadir S, Das J, Bosak S, Prajapat M. The study of simultaneous bilateral ocular trauma in Northern India: clinical presentation, epidemiology and patterns of injury. Int Ophthalmol. 2021;42(4):1193-203. [Google Scholar]
- Maurya R. Ocular trauma during COVID- 19 crisis: Trends and management. Indian J Clin Exp Ophthalmol. 2020;6(4):478-9. [Google Scholar]
- Marudhamuthu E, Sivakumar N, Kumaravel T. Studyofocularinjuries in road traffic accident patients. J Eval Med Sci. 2017;6(41):3219-22. [Google Scholar]
- Desai P, Macewen C, Baines P, Minassian D. Incidence of cases of ocular trauma admitted to hospital and incidence of blinding outcome. Br J Ophthalmol. 1996;80:592-6. [Google Scholar]
- Kaur A, Agrawal A. Paediatric Ocular Trauma. Curr Sci. 2005;89(1):43-6. [Google Scholar]