IP International Journal of Ocular Oncology and Oculoplasty
Official Publication of Khyati Education And Research Foundation
Official Publication of Khyati Education And Research Foundation
Author Details :
Volume : 5, Issue : 1, Year : 2019
Article Page : 34-37
https://doi.org/10.18231/2581-5016.2019.0009

Abstract
Basal cell carcinoma is the most common skin cancer mainly caused by prolonged exposure to ultraviolet rays. It is also known as rodent ulcer or basal cell epithelioma. Pigmented basal cell carcinoma is a rare variety of basal cell carcinoma. It typically affects older age group. Most important risk factors are fair skin, inability to tan, and chronic exposure to sunlight. 90% of cases occur in head and neck and about 10% of these involve the eyelids. It is the most common malignant eyelid tumour, accounting for 90% of all cases, most frequently arises from lower eyelid followed by medial canthus, upper eyelid and lateral canthus. Among all variant of BCC, pigmented BCC variety is about 6%. Histopathologically, it is similar to nodular BCC with increased melanisation.
we report a rare case of pigmented BCC that we encountered in our setup.
Keywords: Basal cell carcinoma, Pigmented basal cell carcinoma, Ultraviolet presentation.
Basal cell carcinoma (BCC) also termed as rodent ulcer is a type of skin carcinoma. It is one of the most common form of human malignancy.[1] It has a lifetime risk of 12%.[2]12% to 16% of BCCs occur on the periocular skin.[3],[4] It is usually a slowly enlarging tumour and symptoms are rare.[5]
It is one of the commonest carcinoma amongst Caucasians but rare among dark skinned peoples. It rarely spreads to other tissues, unlike melanomas. Basal cell carcinoma usually spreads to the surrounding skin. Although this is generally slow, failure to get an appropriate treatment can lead to a considerable area of skin being destroyed and thus requiring plastic surgery.[5] It typically affects older age group. Most important risk factors are fair skin, inability to tan, and chronic exposure to sunlight. 90% of cases occur in head and neck and about 10% of these involve the eyelids. It is the most common malignant eyelid tumour, accounting for 90% of all cases, most frequently arises from lower eyelid followed by medial canthus, upper eyelid and lateral canthus. It is a slow growing, locally invasive but non metastasizing tumour.[1] Tumour near the medial canthus are more prone to invade orbit and sinuses and it is difficult to manage apart from the tumour arising from elsewhere and also carry the greater risk of recurrence. Tumour that recur following incomplete treatment tend to be more aggressive.[1]
Among all variant of BCC, pigmented BCC variety is about 6% and histopathologically it is similar to nodular BCC with increased melanisation.[6]
This case report describes a rare case of pigmented BCC that we encountered in our setup.
A 80-year-old male patient, farmer by occupation came with complaints of ulceration of lower eyelid and nasal crease on the left side since 1 years (Fig. 1). He had not taken any treatment for same. There was gradual increase in size of the ulcer. No history of bleeding or discharge from an ulcer.
On examination, there was a single ulcer over left upper “eyelid” 5 cm × 3 cm with rolled out edges without any bleeding or discharge and ulcer was not fixed to the underlying structure (Fig. 1). Investigations revealed, hemoglobin 12 g%, total leukocyte counts 6700/cu.mm, platelets 2.04 lac/cu.mm, random blood sugar 105 mg/dl.
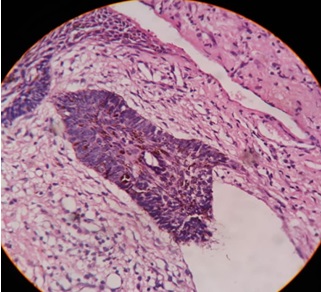
Histopathological examination was done. H and E stain of section of left lower eyelid in the left medial canthus near the nose showed on one slide the covering being stratified squamous epithelium and was acanthotic, on focus the tumor cells were found in islets. The tumor composed of basaloid cells, with palisading of similar basaloid cells with hyper chromatic pleomorphic nuclei surrounding the central area of cells. Melanin pigments and melanophages were seen along with massive infiltration of neutrophils with necrotic debris and bacterial colonies. These findings confirmed the diagnosis of pigmented BCC (Fig. 2).
The patient was advised for MRI of the orbit and face with contrast study. It showed the presence of a solid lesion n the left side of the face, infraorbital region adjacent to the medial cants of the left eye. The lesion involved the skin and subcutaneous fatty tissue. Inferior eyelids were involved. The muscle layer was spared. No extension of the lesion into the orbit or the paranasal sinuses. It measured 10 mm in AP and 25 mm in transverse and 27 mm in craniocaudal diameters (Fig. 3).
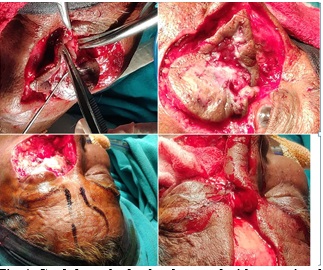
Once confirmed, wide excision with full thickness skin grafting was performed. Graft was harvested from the forehead and later the donor site was covered with a rotational paramedic flap (Fig. 4). The remaining defect was covered by Mustarde cheek rotational flap (lower eyelid defects are reconstructed using a mustarde cheek rotational flap. This large skin muscle flap is rotated from the cheek to repair large lower eyelid defects) (Fig. 5). Patient was followed on first post operative day and seventh post- operative day. Post-operative follow- up on 7th day showed healthy wound margins. The patient was advised for suture removal on 14th day. Further flap detachment and lid reconstruction has been planned on 21st post-op day.
 |
Click here to view |
Fig. 1: Single ulcer over left upper “eyelid” 4 cm × 3 cm with rolled out edge.
 |
Click here to view |
Fig. 2: pigmented BCC.
 |
Click here to view |
Fig. 3: MRI of the orbit and face
 |
Click here to view |
Fig. 4: Graft from the forehead covered with a rotational paramedic flap.
 |
Click here to view |
Fig. 5: Mustarde cheek rotational flap.
 |
Click here to view |
Basal cell carcinoma represents the most common form of skin cancer, accounting for 90% of the eyelid malignancies.[7] Basal cell carcinomas rarely metastasise, they can be locally destructive and leads to significant morbidity, especially when located in the periocular area.[8] Histologically aggressive basal cell carcinoma (Subtypes-infiltrative, micronodular and basosquamous) has a higher rates of recurrence and also has an increased risk of perineural and perivascular invasion.[9]
Histological subtypes of basal cell carcinoma
The classifications of the histological subtypes advocated by the Royal College of Pathologists and the World Health Organisation have been widely adopted in the recent literatures.[10],[11]The growth patterns (superficial, nodular, infiltrative and micronodular) and are among the main growth patterns idetified, the infiltrative and micronodular subtypes being associated with significantly increased risk of local recurrence and overall morbidity.[11] Nodular basal cell carcinoma is known to occur more frequently on the head and neck, whilst infiltrative basal cell carcinoma preponderates over superficial basal cell carcinoma on the face.[12][13],[14],[15],[16]Hence the significance of this carcinoma in the periocular region is of utmost importance as it has a higher rate of local invasion and hence may require aggressive treatment as compared to standard treatment. BCC has a tendency to grow slowly. It is rare for a basal cell carcinom to metastasize to a distant organ. However, if left untreated, it may invade the nearby tissue and further may invade the deeper tissues including muscle and bone.
After treatment, there is a possibility of Recurrence of BCC at the same site. The only peculiar character of BCC is its recurrence in new places in the previously affected individuals. 50% patient with previously diagnosed BCC have a chance to develop a new skin lesion within 5 years.[17],[18]
BCC mostly occur as a single lesion in sun-exposed areas that includes, the angle of the eye below Ohngren’s line. It can also be associated with conditions such as Bowen’s disease, keratoacanthoma, leukoplakia, queyrat erythroplasia, radiation dermatitis[17]and xeroderma pigmentosum.[18]
BCC, can also occur as a feature of hereditary conditions like nevoid BCC syndrome also known as Gorlin’s syndrome[19],[20]or Bazex’s syndrome, Rombo syndrome and unilateral basal cell nevus syndrome. Nevoid BCC syndrome is an inheritant autosomal dominant condition, characterized by a range of developmental anomalies and a predisposing condition to various tumors. Patient with Gorlin’s syndrome mostly presents with a broad nasal root, low intelligence, multiple jaw cysts, palmar pits.[20]
In this patient, the diagnosis pointed towards BCC. On the basis of history taking, clinical examination and investigations we ruled out the possibility of all the syndrome. The patient was operated and managed with wide excision and full thickness skin graft.
BCC tend to occur in a syndrome complex, associated with a number of autosomal dominant inherited disorders and hence prior to the management of the same, the presence of the syndrome must be ruled out.
Acknowledgment
We would like to thank Dr. Biswaranjan Behera, Asst. Prof., Dept. of radiology, Hi- tech medical college and hospital, Bhubaneswar and Dr. Bijaylaxmi Behera, Intern, Department of Surgery, Hi- tech medical college and hospital, Bhubaneswar for helping us.
Abbreviations: BCC- Basal cell carcinoma, H and E- Haematoxylin and eosin, AP- Antero-posterior
Conflict of Interest: None.
How to cite : Rattan A, Rath B, U.khan Z, Chiranjibi C, Subham S, Pigmented basal cell carcinoma: A rare case report. IP Int J Ocul Oncol Oculoplasty 2019;5(1):34-37
This is an Open Access (OA) journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
![]()
![]()
Viewed: 2620
PDF Downloaded: 574