IP International Journal of Ocular Oncology and Oculoplasty
Official Publication of Khyati Education And Research Foundation
Official Publication of Khyati Education And Research Foundation
Author Details :
Volume : 5, Issue : 1, Year : 2019
Article Page : 5-11
https://doi.org/10.18231/2581-5016.2019.0002

Abstract
Introduction: Ophthalmic complications are very common in tuberculous meningitis (TBM) patients, understanding the ocular problems in tubercular meningitis patients is very important for ophthalmologists to intervene on time to prevent irreversible damage to eye.
Hence this investigation has been undertaken to study ophthalmic manifestations in suspected tubercular meningitis patients in both Pediatric and adult population in Basaveshwara teaching and general hospital, Kalaburagi attached to Mahadevappa Rampure Medical College (MRMC).
Materials and Mathods: The study was conducted at Basaveshwara Teaching and General Hospital, Kalaburagi attached to M.R. Medical College, from Dec 2011 to May 2013. 100 admitted patients diagnosed with TB meningitis, were selected for the study. The patients were divided into 2 groups.
Group A consisted of TBM patients who were conscious and cooperative for ophthalmic examination. Group B consisted of TBM patients who were in a state of coma, uncooperative for ophthalmic evaluation.
Results: Out of the 100 patients, 64% had ocular findings. In our study 22% had cranial nerve palsy. Fundus changes were seen in 50% of the patients. Around 22% patients had visual acuity, CSF protein content was considerably high in all patients. Hydrocephalous was seen in 31% (20) patients.
Conclusion: In our study it was observed that most of TBM patients had ocular findings, CSF protein was found in many patients and after treatment there was improvement in ocular problems. We suggest further research with larger sample size to support our findings.
Keywords: Meningitis, Tuberculosis, Ophthalmic manifestations.
Tuberculosis (TB) is still increasing in India at an alarming rate. The most serious form of tuberculosis is tubercular meningitis (TBM). [1]
TBM causes many complications in both children and adult patients. The close association between optic nerve and meninges produces many ocular problems. Commonly found ophthalmic complications in TBM are Optic neuritis, optic atrophy, papilloedema. It may be associated with lid retraction, tonic deviation of eyes, and pupillary abnormality in size. Patients with high CSF protein content are prone for primary optic atropy. Choroidal tubercles and papilloedema are signs of grave complications. [2]
Ophthalmic complications are very common in tuberculous meningitis patients, so understanding the ocular problems in tubercular meningitis patients is very important for ophthalmologists to intervene on time to prevent its irreversible damage to the eye.
Hence this study of ophthalmic manifestations in tubercular meningitis patients has been carried out to know the type of ophthalmic complications present in TBM patients.
The study was conducted at Basaveshwara Teaching and General Hospital, Kalaburagi attached to M.R. Medical College. The study period was from Dec 2011 to May 2013. 100 admitted patients referred from the Medicine, Pediatrics and Neurology department, diagnosed with TB meningitis, were selected for the study.
Out of 100 cases selected, 80 were in the adult age group and 20 were from Pediatric age.
Inclusion Criteria
Exclusion Criteria
A meticulous history was taken from all the cases, followed by a thorough ocular examination.
Observations were made on the modes of presentation and a criterion was applied for diagnosis and the visual outcome in the individual patients.
The following investigations were done in all patients
Methods for clinical examination of the eye
Children below the age of three and those unco-operative for vision were tested depending upon whether they reacted to the light source and whether they followed the light source projected onto their eyes, thus confirming their ‘PLPR’ status (perception of light-PL; projection of rays-PR).
For patients where visual acuity couldn’t be tested (unconscious/ventilated), outcome was based upon their pupillary reactions and their fundus findings.
A little older children and those co-operative for vision were tested by Snellens chart or were tested depending upon whether they followed the light/objects in front of them.
Their families were asked about the child’s facial recognition, social smile and how he responded to objects at home.
Treatment of tubercular meningitis
All patients in the pediatric age group, diagnosed with TBM were given the following treatment.
Prior to starting the treatment, following investigations were done-
Treatment
Intensive phase consisted of 4 drug combination- HRZE
H- Isoniazid: 10 mg/kg/day
R- Rifampicin; 10 mg/ kg/day.
Z- Pyrazinamide: 20 mg/kg/day
E- Ethambutol: 25 mg/kg/day.
After the intensive phase was completed three drug combinations consisting of HRZ was continued for a period of 7 months.
Follow-up
The patient was reviewed after 15 days of discharge from the hospital and called in every month thereafter till the course of treatment was completed.
LFT was done after 15 days of starting on ATT drugs and repeated at 1 month follow-up.
Treatment regime in adults
After the routine investigations were done (as mentioned above) and the patient diagnosed as TBM, the following treatment was started:
H—300mgOD
R—600rngOD
Z-l.5 gOD
E—1.5 mg/kg/day’.
If the weight of the patient is < 30>
Follow- up
Patients were called for a monthly follow up and then bi-rnonthly follow up till the symptoms subsided.
Statistical Analysis
Results
A total of 100 admitted patients diagnosed with tubercular meningitis were taken up for this study.
The patients were divided into 2 groups.
Group A consisted of TBM patients who were conscious and cooperative for ophthalmic examination.
Group B consisted of TBM patients who were in a state of coma, uncooperative for ophthalmic evaluation
Table 1: Total study group patients divided into groups
|
Group |
Patients |
Percentage |
|
A |
88 |
88 |
|
B |
12 |
12 |
|
Total |
100 |
100 |
Out of the 100 patients, 64% had ocular findings: Out of the 88 patients in group A, 52(59.09%) patients had ocular manifestations and remaining 36 (40.9%) showed no ocular manifestations.
Table 2: Age & sex wise distribution of study population
|
Age |
Sex |
Total |
% |
|||
|
Males |
% |
Females |
% |
|||
|
0-14 |
16 |
31.4 |
14 |
28.6 |
30 |
30 |
|
15-20 |
04 |
7.84 |
10 |
20.4 |
14 |
14 |
|
21-30 |
11 |
21.6 |
16 |
32.6 |
27 |
27 |
|
31-40 |
09 |
17.6 |
05 |
10.4 |
14 |
14 |
|
41-50 |
05 |
9.80 |
02 |
4.08 |
07 |
07 |
|
51-60 |
06 |
11.8 |
02 |
4.08 |
08 |
08 |
|
Total |
51 |
100 |
49 |
100 |
100 |
100 |
Males constituted 51(51%) of the total cases while females constituted 49(49%). Majority i.e 55(55%) were in the age group between 15-40 years of age. 30(30%) were in the pediatric age group and 15(15%) were in the age group between 4 1-60 years. Mean age of males is 24.26±12.52 Mean age of females is 24.404±13.64As the p> 0.05, the difference in the age distribution of cases among males and females is not significant.
Table 3: Visual acuity of study population
|
S. No |
Visual acuity |
Total |
Percent |
|
1 |
6/6-6/8 |
61 |
61 |
|
2 |
<6> |
10 |
10 |
|
3 |
<6> |
05 |
5 |
|
4 |
<3> |
07 |
7 |
|
5 |
NO PL |
05 |
5 |
|
6 |
Not rec. |
12 |
12 |
|
|
Total |
100 |
100 |
Table 4: Cranial nerve palsy in study populations
|
S. No |
Cranial nerve |
Male |
Female |
Total |
|
1 |
III: Complete Incomplete |
1 |
1 |
6 |
|
2 |
2 |
|
||
|
2 |
VI: Unilateral Bilateral |
6 |
6 |
13 |
|
1 |
0 |
|||
|
3 |
VII |
00 |
01 |
01 |
|
4 |
Combined |
02 |
04 |
06 |
|
|
Total |
10 |
10 |
22 |
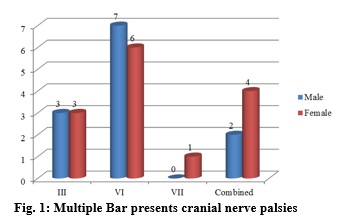
Cranial nerve palsy was seen in 22(22%) patients
Combined nerve palsy was often seen in association with 2’nerve involvement (5out 6).
II and VI nerve constituted 4 patients
II and III nerve constituted 2 patients
III and VI nerve involvement was seen in 1 patient.
The p value is more than 0.05 which shows that there is no significant difference in the cranial nerve palsies between males and females.
 |
Click here to view |
Fig. 1: Multiple Bar presents cranial nerve palsies
Table 5: Fundus findings
|
S. No |
Features |
Patients |
Total |
% |
|
1. |
Normal |
50 |
50 |
50 |
|
2. |
Papilloedema |
21 |
21 |
21 |
|
3. |
Papillitis |
12 |
12 |
12 |
|
4. |
Temporal pallor: Bilateral |
05 |
05 |
05 |
|
5. |
Total OA: Primary Secondary |
05 07 |
12 |
12 |
|
|
Total |
100 |
100 |
100 |
Fundus changes were seen in 50(50%) of the patients. Papilloederna was seen as the most common finding, in 21% of patients and Papillitis constituted 12%.
Blindness occurring secondary to optic atrophy. Optic atrophy occurred as post-papilloedema/papillits (secondary) or as primary optic atrophy.
Optic atrophy was either complete (total pallor of disc) or incomplete (temporal pallor).
Table 6: Pupillary findings
|
S. No |
Pupillary changes |
No |
% |
|
1 |
Sluggish |
27 |
56.25 |
|
2 |
Anisocoria |
03 |
6.25 |
|
3 |
Fixed dilated |
02 |
4.17 |
|
4 |
RAPD (grade 3-4) |
16 |
33.33 |
|
|
Total |
48 |
100 |
Table 7: Visual field changes
|
S. No |
Visual field findings |
Patients (n) |
% |
|
1 |
Normal |
34 |
34 |
|
2 |
Enlargement of blind spot |
5 |
5 |
|
3 |
Peripheral constriction |
6 |
6 |
|
4 |
Scotoma |
4 |
4 |
|
5 |
Not recordable |
15 |
15 |
|
6 |
Not done |
36 |
36 |
|
|
Total |
100 |
100 |
The above findings were in regards to the worse affected eye. Out of the 100, static perimetry was done only in patients with stage II and III.
Out of the 64 patients, in 34 patients, perimetry was normal. 5 patients showed enlargement of blind spot.
6 patients showed peripheral constriction of the visual field.
3 patients showed central scotoma and 1 patient showed centrocecalscotoma.
In 15 patients, perimetry could not be recorded because they were in stage III, unco-operative/ unconscious state and those who showed complete optic atrophy, visual field testing is not possible.
Table 8: CSF findings
|
S.no |
CSF parameters Patients (n) |
Patients (n) |
Percentage |
|
|
1 |
Protein (mg/1) |
|
|
|
|
|
a) <50> |
0 |
0 |
c12=12.35 (p<0 p=0.01> significant |
|
|
b)51-100 |
8 |
8 |
|
|
|
c) 101-300 |
|
|
|
|
|
d)>300 |
|
|
|
|
2 |
Glucose (mg/dl) |
|
|
c2=14.86 (p<0> |
|
|
a) 0-40 |
80 |
80 |
|
|
|
b)41-70 |
17 |
17 |
|
|
|
c) >70 |
3 |
3 |
|
|
3 |
Cells/mm3 |
|
|
c2=11.76 (p<0> |
|
|
a)0-20 |
0 |
0 |
|
|
|
b) 21-100 |
50 |
50 |
|
|
|
c) 101-200 |
18 |
18 |
Significant |
|
|
d) 201-300 |
20 |
18 |
|
|
|
e) >300 |
12 |
12 |
|
|
4 |
Low CSF chloride (<19> |
67 |
67 |
|
A lower level of glucose (<40>70mg/dl
The mean value of glucose was 80% of the cases who had a cobweb appearance of CSF and protein was found to be elevated in all cases.
27 cases had >300 mg CSF protein, max being 2g.
The mean value of protein was CSF cells were elevated in all cases
All cases had >60% lymphocyte predominance.
Table 9: CT scan findings
|
S.no |
CT Findings |
No. of Patients |
|
1 |
Normal |
32 |
|
2 |
Hydrocephalus |
21 |
|
3 |
Basal exudates |
5 |
|
4 |
Basal infarcts |
5 |
|
5 |
Tuberculoma |
1 |
|
6 |
Cerebral edema |
2 |
|
7 |
Not done |
34 |
CT scan was done in 66 patients. Out of the 66 patients, maximum patients i.e 21(31.8%) had Hydrocephalus.
Basal Meningitis was seen in 10(15.15%) patients.
Tuberculorna was found in 1(1.51%) patient.
Cerebral edema was seen in 2(3.03%).
CT scan was not done in 34 patients.
Table 10: Risk factors for potential ocular abnormalities
|
S. No |
Risk factors |
No. of cases |
Percentage |
|
1 |
Delayed presentation |
64 |
64 |
|
2 |
Protein levels |
|
|
|
|
<05> |
0 |
0 |
|
|
51-100- |
8 |
8 |
|
|
100-300- |
65 |
65 |
|
|
>300- |
27 |
27 |
|
3 |
Hydrocephalous |
20 |
20 |
|
4 |
Interrupted treatment |
1 |
1 |
The above table shows that more than half of the patients had ocular manifestations. i.e 64 out of 100 patients
The protein content was considerably high in all patients
Hydrocephalous was seen in 20 patients.
|
Risk factor |
Group A Mean±S.D |
Group A2 Mean±SD |
Group B Mean±SD |
t-test and p comparsion |
|
CSF Sugar |
33.80±15.5 |
30.5±12.46 |
33.0±17.12 |
A1&A2:p>0.0 A2&B:p>0.0 A1&B:p>0.0 |
|
CSF Protein |
128.67±125.75 |
283.58±157.82 |
549.5±122.14 |
A1&A2:p>0.0 VHS A2&B:p>0.0 A1&B:p>0.0 P<0> |
|
CSF Cells/mm |
92.27±46.37 |
171.23±123.82 |
249.41±103.95 |
A1&A2: p>0.001; VHS A2&B:p>0.0 A1&B: p>0.001, VHS |
|
CSF chloride |
17.55±10.75 |
90.96±25.3 |
96.58±17.46 |
A1&A2: p>0.001; VHS A2&B:p>0.0 A1&B: P<0> VHS |
|
CSF ADA |
13.0±6.63 |
13.59±7.3 |
16.98±5.38 |
A1&A2: p > NS AD&B: P<0> A1&B: p<0> |
|
Hydrocephalus |
0 |
12 |
9 |
c2=17.5, p<0> |
The above table shows the comparison of risk factors for oculo-visual anomalies between the three groups.
Group A has been divided further into Al & A2 where Al consists of 36(36%) patients without any ocular manifestations.
A2 consists of 52(52%) patients with ocular manifestations. It is clear that there is significant difference in the severity of risk factors between the groups with group B having a
higher risk of ocular anomalies than group A and Group A2 a higher risk than Al.
S- Significant
HS- Highly Significant
VHS- Very Highly Significant
NS- Not Significant.
Table 11: Visual outcome after treatment
|
S. No |
Visual acuity |
At 1 month |
At 3rd month |
|
1 |
>6/18 |
69 |
66 |
|
2 |
< 6> |
18 |
14 |
|
3 |
< 6> |
18 |
14 |
|
|
No PL |
7 |
8 |
|
|
Total patients |
94 |
88 |
Six patients were lost (death) during the period of stay in the hospital, thus only 94 patients were available for 1 month follow-up.
At 3’ month, additional 6 patients were lost as they did not turn up for follow-up visit. Thus 3’’ month follow up included 88 patients.
|
S. No |
Fundus |
At 1 month |
At 3rd month |
|
1 |
Papilloedema |
5 |
0 |
|
2 |
Papillitis |
12 |
0 |
|
3 |
Partial optic atrophy |
3 |
9 |
|
4 |
Total optic atrophy |
7 |
8 |
|
|
Total |
94 |
88 |
Group wise comparison of outcome
|
Visual outcome |
Group A |
Group B |
Total |
|
Normal |
29 |
0 |
29 |
|
Improved |
38 |
0 |
38 |
|
Not improved |
14 |
7 |
21 |
|
Expired |
1 |
5 |
6 |
|
Did not turn up |
6 |
0 |
6 |
|
Total |
88 |
12 |
100 |
The above table shows that mortality rate and poor visual outcome is more amongst group B population. i.e Stage III of Tubercular Meningitis. Out of the 12 patients who presented in stage III, 5(41.66%) expired during their stay at the hospital and 7(58.33%) had oculovisual anomalies.
c2= 15.26, p
In our study out of 100 TBM patients 64% had ocular manifestations, Verma et al,[3] investigated 50 cases of pediatric tubercular meningitis, they observed that 76% had ophthalmic problems. There was frequent involvement of third nerve and sixth cranial nerve. It’s been observed that highest incidence of mortality was with sixth nerve palsy which is followed by a complete third canial nerve palsy.
In our study 22% had cranial nerve palsy in that 13% had 6 nerve palsy and 6% had 3rd nerve palsy, Lamba PA et al carried out a study on 48 children with TBM, in which Optic disc changes (papillitis) constituted 62%, papillary involvement was in 48% of patients and cranial nerves (3rd) involvement was found in 28% of patients.[4]
22% had visual acuity, 21% had papilloedema, 12% had papillitis Mishra M, et al, carried out study on 100
patients with T.B. meningitis, 82% of patients had ocular complications in which 40% presented with diminished visual acuity, 22% had papilloedema, 25% presented with ocular paresis, 18% had pale disc and 10% choroidal tubercles.; 22% had evidence of obstructive hydrocephalus diagnosed by ventriculogram/C.T, 20% cases had vasculitis
diagnosed by angiography and 12% of patients had Tuberculoma.[5]
In our findings 80% percent showed low level of CSF glucose, 27 cases had CSF protein more than 300mg and CT scan was done in 66 patients out of this 21(31%) had hydrocephalus, basal meningitis was seen in 15%, tuberculoma was observed in 1.5% and cerebral edema was found in 3% of patients. Sinha et al, conducted study on 101 patients of T.B. meningitis, in which at the study enrolment 74 patients had normal vision and 27 patients presented with low vision. During the process of study 13 patients died and
remaining 88 patients who survived at 6 months, in 88 survived patients 68 patients had good vision, 11 patients presented with low vision and 9 patients had presented with blindness. Papilloedema, cranial nerve palsies, raised cerebrospinal fluid protein (> 1 g/L), and presence of optochiasmatic arachnoiditis in MRI diagnosis were predictors of vision deterioration. The predictors of blindness at 6 months were observed to be papilledema, vision acuity < 6/18, cranial nerve palsies, tuberculous meningitis stage II or III, raised cerebrospinal fluid protein (> 1 g/L), optochiasmatic arachnoiditis, and optochiasmal tuberculoma.[6]
Benneggi A et al, found a case with severe ocular manifestations in a patient with tuberculous meningitis.[7]
Anupriya A et al carried out a study on 163 patients and had observed that Optochiasmatic Arachnoiditis may occur as a complication of T.B. meningitis.[8]
Smith et al, found that tuberculosis was mediating factor in acquired abducens nerve palsy in children.[9]
In our investigation visual acuity improved from 1month post-operative period to 3rd month post-operative period, fundus changes like papilloedema and papillitis became nil after 3rd month post-operative period. Mortality rate and poor visual outcome was found more amongst stage III TBM patients. It is clear that there is significant difference in the severity of risk factors between the groups with group B having a higher risk of ocular anomalies than group A.
In our study it was observed that most of TBM patients had ocular findings. Timely intervention for TBM can prevent severity of ocular problems. We suggest further research with larger sample size to support our findings
Conflict of interest: None.
Financial support: None.
How to cite : Reddy R, Munoli K, Patil A, Study of ophthalmic manifestations in tubercular meningitis patients. IP Int J Ocul Oncol Oculoplasty 2019;5(1):5-11
This is an Open Access (OA) journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
![]()
![]()
Viewed: 3346
PDF Downloaded: 624