IP International Journal of Ocular Oncology and Oculoplasty
Official Publication of Khyati Education And Research Foundation
Official Publication of Khyati Education And Research Foundation
Author Details :
Volume : 5, Issue : 1, Year : 2019
Article Page : 1-4
https://doi.org/10.18231/2581-5016.2019.0001

Abstract
Introduction: To determine the association between subclinical hypothyroidism and diabetic retinopathy in type 2 diabetic patients.?
Study design: cross sectional (observational) study.
Place and Duration of Study: 1. The Retina Clinic, Institute of Ophthalmology, Jawaharlal Nehru Medical College, A.M.U., Aligarh. 2. Rajiv Gandhi Centre for Diabetes and Endocrinology, Jawaharlal Nehru Medical College, A.M.U., Aligarh, from January 2017 to February 2018, Materials & Methods: Total 60 patients with diabetes mellitus II were enrolled.30 patients with diabetic retinopathy were taken as cases, while a similar number of patients without diabetic retinopathy were taken as controls. Known patients of type 1 diabetes mellitus (T1DM), autoimmune disorders, pregnancy, chronic renal failure and chronic liver disease, Malignancies or history of chemotherapy or radiotherapy within past 1 year were excluded from the study. Serum free T3, T4 and serum TSH were measured by Beckman Coulter, Access 2, which uses the chemiluminescence immunoassay technique.
Statistical Formula: SCH was compared between case and control groups using chi square test. Odds ratio was also calculated for SCH. p value <0>
Results: Cases (group A) had higher mean serum TSH as compared to controls (group B). SCH was diagnosed in 16 individuals (13 cases and 03 controls). Overall prevalence of SCH was 26.67% (43.33% in group A and 10% in group B). Pearson Chi square test revealed significantly higher prevalence of SCH in group A (p value 0.004). OR was 2.103 (CI 1.354 – 3.267).
Conclusion: There was significant association between SCH and DR in type 2 diabetic patients.
Keywords: Diabetic retinopathy, Subclinical hypothyroidism, Type 2 diabetes mellitus.
Diabetes mellitus and the eye diseases connected with it comprise a set of complex disorder with multi factorial etiology, where both genetic and environmental factors play an active role. It is a substantial cause of environmental blindness in both the developed and developing countries. Newly diagnosed diabetic cases are increasing at an alarming rate in the developing countries like India due to better lifestyles and demographic right shift of the population, urbanization and differences in the access to the health care system. “Approximately, 382 million people across the world have been estimated to have been DM in 2013 and if no action is taken this number will rise to 592 million by 2035. WHO estimates that 19% of the worlds diabetic population lives in India and 80 million people in India will have Diabetes by the year 2030”.[1]
“DR at present affects almost 100 million people worldwide and is set to become an ever-increasing health burden, with estimates between 1990 and 2010 showing that DR-related visual impairment and blindness increased by 64% and 27%, respectively [2]”
Thyroid diseases and diabetes mellitus are the two most common endocrine disorders encountered in clinical practice. Diabetes and thyroid disorders have been shown to mutually influence each other and a connection between both conditions has been reported in literature.[3]
Thyroid disease is a pathological state that can adversely affect glycemic control in diabetics and has the potential to affect the health. Thyroid disease is found commonly in diabetes and is associated with advanced age, particularly in type 2diabetes and underlying autoimmune disease in type 1diabetes.[4] Insulin and thyroid hormones are intimately involved in cellular metabolism and thus excess or deficit of either of these hormones result in the functional derangement of the other. The physiological and biochemical interrelationship between insulin and the influence of both insulin and iodothyronines on the metabolism of carbohydrates, proteins and lipids are recorded. Such findings indicate that iodothyronines are insulin antagonist with high levels being diabetogenic while absence of the hormone inhibits the development of diabetes.[5] The thyroid hormone replacement is associated with a fall in glycosylated haemoglobin (HbA1c) level, which is influenced by increased erythropoiesis rather than by changes in glucose level.[6]
The prevalence of SCH is 4–9% in the general population and our data suggests the same prevalence to be about 10.2% in T2DM population.[7],[8],[9],[10],[11] Numerous studies propound that SCH is associated with hypertension, high cholesterol, and abnormal homocysteine level and patients with SCH have a higher risk of metabolic syndrome, atherosclerosis, cardiovascular events, and mortality.[12],[13],[14]
The mechanism behind the association between DR and SCH may be the fall in circulating IGF-1, which is integral for a normal retinal vasculature, and the decrease of IGF-1 may be mediated by thyroid dysfunction.[15]
Aim of our study was to find out the influence of SCH on diabetic retinopathy. If any connection between two exists, then routine screening or more frequent follow ups for thyroid patients may be considered desirable in type 2 diabetic subjects. This may also be helpful in investigating new tactics for preventing the development and/or progression of retinopathy.
This cross-sectional study was conducted after taking ethical clearance from Institutional Ethical Committee, Jawaharlal Nehru Medical College and Hospital, A.M.U, Aligarh. Tenets of the Declaration of Helsinki were followed. An informed written consent was taken from each patient and\or patient attendant before participation in the study. The study population was drawn from the diabetic patients who attended the Rajiv Gandhi Center for Diabetes and Endocrinology, and subsequently were referred to the Retina Clinic, Institute of Ophthalmology, of the same hospital, for their ocular evaluation.
A clinical history was taken with the help of a structured questionnaire on a specially designed Performa (Appendix) including- demographic data, duration of diabetes, treatment taken, presence of any other complications of diabetes, addictions, dietary habits, family history of diabetes, and blood pressure.
The laboratory profile of each patient comprised of Blood sugar (both fasting greater than or equal to 126mg/dl in diabetes), HbA1C (greater than or equal to 6.5% in diabetes), thyroid hormones (reference range values serum T3 1.2 – 2.8 nmol/L, serum T4 60 – 160 nmol/L, serum TSH 0.17 – 5.0 mIU/L). The Thyroid profile was assessed by Beckman Coulter, Access 2, which uses the chemiluminescence immunoassay technique.
Total 60 patients with diabetes mellitus II were enrolled. 30 patients with diabetic retinopathy were taken as cases, while a similar number of patients without diabetic retinopathy were taken as controls. Known patients of type 1 diabetes mellitus (T1DM), autoimmune disorders, pregnancy, chronic renal failure and chronic liver disease, major depressive disorder, medications affecting thyroid hormones, Malignancies or history of chemotherapy or radiotherapy within past 1 year were excluded from the study.
A diagnosis of diabetic retinopathy was made when a patient exhibited a minimum of one microaneurysm in any field, as well as hemorrhages (dot, blot or flame shaped) and maculopathy (with or without clinically significant macular edema). The diagnosis of proliferative diabetic retinopathy was made only if there is neovascularization.
SPSS version 20 was used for analysis. Continuous variables were expressed as means, standard deviation (SD) and range. Independent and, paired t test were used as per the type of data. Non parametric, discrete data were evaluated using Chi square. Odds ratio was used to quantify the strength of association. Levene’s test was used to assess the equality of variances for a variable calculated across the two groups. The difference was considered significant at a p value of <0>
60 type 2 diabetic subjects satisfying the inclusion criteria were selected from the individuals reporting at Rajeev Gandhi Centre of Endocrinology and Institute of Ophthalmology, Aligarh Muslim University, Aligarh and categorized into group A (cases) and group B (controls).
The clinical characteristics and biochemical data of the study participants are summarized in table I
Out of the 30 cases in group A (cases), 18 (60%) were female and 12(40%) were male. Among 30 individuals in group B (controls), 16 (53%) were female and 14 (46%) were male (Table-1). Mean age was 53.36 ± 7.69 years in cases and 53.89 ± 7.93 in controls. Descriptive statistics (Mean ± SD) for quantitative variables like age, HbA1c, serum TSH, free T3 and free T4 were measured for both groups as shown in table I and it revealed that Group A (cases) had higher mean serum TSH as compared to group B (controls).
SCH was diagnosed in 16 individuals (13 cases and 03 controls). Overall prevalence of SCH was 19.9% (24.3% in group A and 15.6% in group B). SCH was compared between the two groups by using Pearson Chi square test and it disclosed significantly higher prevalence of SCH in group A (p?0.05) as shown in table-2. Odds ratio was 1.738 (CI 1.129 – 2.917).
Table 1: Clinical characteristics and biochemical data of study participants
|
Variable |
Control (n= 30) |
Cases (n= 30) |
p- value |
|
Age (years) |
51.43 |
53.75 |
p>0.05 |
|
HbA1c (%) |
7.39±1.16 |
8.215±1.81 |
p<0> |
|
Serum free T4 (nmol/L) |
116.03 |
112.506 |
p>0.05 |
|
Serum TSH (mIU/L) |
3.13 |
5.41 |
p<0> |
Table 2: Comparison of SCH status according to biochemical cut offs in cases and control & risk estimate of diabetic retinopathy due to SCH (n = 60)
|
Subclinical Hypothyroidism |
Controls |
Cases |
|
Yes |
3 (10) |
13(43.3) |
|
No |
27 |
17 |
 |
Click here to view |
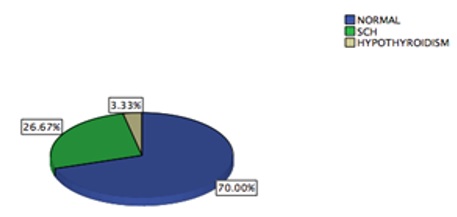
Fig. 1 Prevalence of Thyroid dysfunction in the two groups of diabetes patients
Discussion
Multiple classification of D.R. have been used in different studies, so that it is often difficult to compare one study with another.[16],[17],[18]
Vision itself may not always be a dependable index of status of retinopathy. For instance, visual acuity may improve following the clearing of vitreous haemorrhage, yet the underlying retinopathy may have deteriorated.[19]
Fairly all patients with T1DM and >60% with T2DM are expected to have retinopathy by the first decade of incidence of D.M.[20]
D.R. is the most consequential cause of blindness for diabetes, accounting 70% of blindness suffered among diabetes.[21]
“With respect to a non diabetic, a diabetic has 11 times greater risk of blindness, and a diabetic with retinopathy has a 29 times greater risk of blindness, among all age groups”.[21]
Recently, association of SCH towards development and/or progression of DR is being looked for in various studies. However, these studies have generated ambiguous results. To the best of our knowledge, this association has not yet been studied in India. The findings of our study demonstrate that there is significantly higher prevalence of SCH in diabetic patients having DR as compared to diabetic patients who have not developed retinopathy. This study also shows increased risk of retinopathy in diabetic patients with subclinical hypothyroidism.
Though most of the cross sectional studies revealed that SCH is independently associated with diabetic retinopathy in type 2 diabetic adults, the outcomes are not correspondingly concordant in all studies. In a case control study on 371 Chinese type 2 diabetic patients, prevalence of SCH in subjects having proliferative DR was 27.3% while it was 17.4% in the subjects without DR.[22]
Added study conducted in Korea showed higher prevalence of DR (32.8%) in SCH diabetic patients than in euthyroid diabetic patients (19.6%) and SCH remained significantly associated with DR, self reliant of other clinical and biochemical factors such as HbA1c, BMI, duration of diabetes, diabetic nephropathy and hypertension.[23]
Parallel in another study conducted on 1,170 type 2 diabetic patients, SCH was found to be associated with higher prevalence of DR especially sight threatening DR (OR=4.15) after adjustment for possible confounding factors. DR was divided according to the risk of loss of vision and it was shown that SCH was also associated with the severity of DR. In this study, euthyroid patients were further divided into two sub-groups (TSH 2.0 - <4>[24]
Akin, a study was carried out in Spain in 2012 to investigate the relationship between SCH and DR in Caucasian population; this study could not establish any relationship between either TSH level or presence of SCH with DR.[25] Although this study did not find any relationship, the range of TSH was from 0.1 to 18.71mIU/l and therefore a potential effect of higher TSH levels on the development of diabetic macular oedema and DR could not be ruled out.
The disputatious outcomes of these studies may be elucidated by the heterogeneity of the participants e.g. differences in race and ethnic groups, age, BMI, duration of diabetes, HbA1c level hypertension and dyslipidemia.
Another imperious consideration in this regard is lack of screening for autoimmunity because relationship of autoimmune diseases and thyroid disorders has been confirmed. The other possible drawbacks include lack of adjustment for some important confounders, limited power for detection of weak associations, random error due to use of single biochemical measurement, and observational study design which makes it nearly impossible to ascertain a causal relationship between SCH and DR in type 2 diabetic subjects. The study population comprised of patients cared for at a single tertiary centre. Henceforth, the results may not be applicable to all Indian patients with type 2 diabetes. So, follow-up thyroid function tests are needed to confirm the association between the clinical course of SCH and diabetic retinopathy. Compared with the studies having a large sample size, studies with a small sample size may overestimate the true association.
The present study provides evidence that SCH is associated with diabetic retinopathy in Indian patients with type 2 diabetes even after controlling for potentially confounding clinical variables. Larger prospective studies are required to confirm the association between SCH and diabetic retinopathy in patients with type 2 diabetes.
How to cite : Ahmed A, Waris A, Anjum A, Sukul R, Faizi N, Correlation between subclinical hypothyroidism and diabetic retinopathy in type 2 diabetic patients. IP Int J Ocul Oncol Oculoplasty 2019;5(1):1-4
This is an Open Access (OA) journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
![]()
![]()
Viewed: 1847
PDF Downloaded: 524