- Visibility 891 Views
- Downloads 80 Downloads
- Permissions
- DOI 10.18231/j.ijooo.2021.004
-
CrossMark

Abstract
Aims: To assess the outcome of lateral tarsal strip (LTS) for the involutional entropion and ectropion.
Materials and Methods: A quasi study was carried out in a tertiary eye hospital of Dhaka, Bangladesh, between January 2013 and December 2020. This study included all patients who underwent lateral tarsal strip (LTS) procedure for the correction of involutional entropion and ectropion. Group A patients were presented with involutional entropion and group B patients were presented with involutional ectropion. We assessed surgical outcome and postoperative complications.
Results: Out of 48 lower eyelids marginal malposition of 43 patients were studied in this study and 5 cases were presented bilateral lower lid marginal malposition. Lateral tarsal strip (LTS) procedure was a unique procedure to correct the involutional entropion (24 eyelids 50%), involutional ectropion (24 eyelids 50%), involving the lower eyelid. The male to female ratio was almost 2.6:1. The mean age was 68.49 years with 54 years to 90 years age range. The surgical correction was satisfactory in 95.9%, and 91.7% of lower eyelids involutional entropion, and involutional ectropion respectively.
Conclusions: Lateral tarsal strip (LTS) is a unique procedure to achieve better cosmetic and functional outcome for the correction involutional eyelid marginal malposition (entropion, and ectropion).
Introduction
Involutional entropion and involutional ectropion are common eyelid malposition. Entropion presents with Inward rotation of the eyelid towards the globe and ectropion causes an outward rotation of the eyelid margin away from the normal eyelid position. There are various surgical options to correct the entropion and ectropion. Quikert’s procedure, wies procedure, Wheelers technique, triangular tarsectomy, wedge excision, wheeler technique, or lateral Bick’s shortening and many more techniques are described in literatures for the management of entropion and ectropion.[1], [2], [3] LTS is a successful procedure for the management of horizontal laxity and as well as lateral canthal laxity in the cases of involutional entropion and ectropion.[2] We attempted to analyse the surgical outcome and postoperative complications of lateral tarsal strip (LTS) procedure for the correction of both involutional marginal malposition (entropion and ectropion) of the lower eyelid.
Materials and Methods
A quasi study was carried out in a tertiary eye hospital of Dhaka, Bangladesh, between January 2014 and December 2020. This study included all patients who underwent lateral tarsal strip (LTS) procedure for the correction of involutional lower eyelid marginal malposition (entropion and ectropion), and followed up after the LTS surgery up to 1 year during the time of January 2013 to December 2020. Group A patients presented with involutional entropion and group B patients were included involutional ectropion. We assessed surgical outcome and postoperative complications. All LTS surgeries were done by a single surgeon. Patients were evaluated clinically, and preoperative general checkup was assessed by an anesthesiologist. Patients with cicatricial entropion, spastic entropion, paralytic ectropion were excluded from this study. We assessed surgical outcome, postoperative complications, and recurrence. Surgical outcome includes restoration of eyelid marginal position nearer to normal eyelid position, and relief of preoperative symptoms. Patients were advised for follow up at 1 month then 3 monthly followed up to one year of surgery. Data were maintained and analyzed statistically using quick calc graph pad software for determination of mean, test of significance and p-value.
Surgical technique for lateral tarsal strip
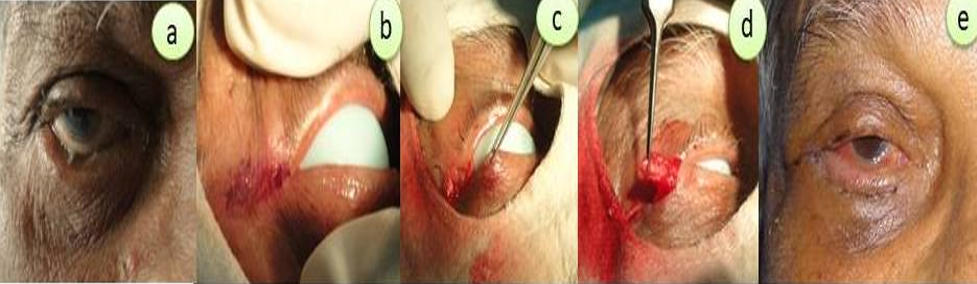
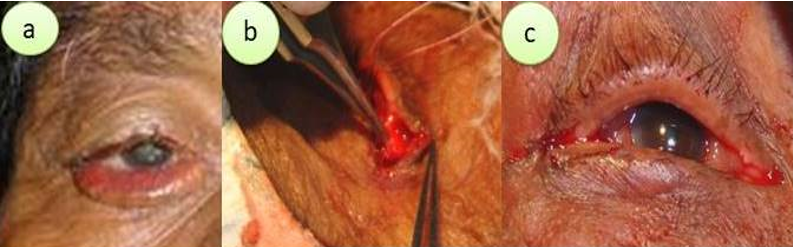
Lateral canthotomy incision about 1 cm is usually made at the lateral canthus by Ellman radiofrequency cautery, then blunt dissection is performed by a straight scissor to expose the periosteum of the lateral orbital wall. An inferior canthotomy and cantholysis was created with RF Cautery with proper hemostasis. Measuring the desired amount of LTS strip with pulled the eyelid towards the lateral canthus. Anterior and posterior lamella of the lateral aspect of lower eyelid is gently separated and then anterior lamella is trimmed to make a LTS strip about 5-10 mm depends on lower eyelid laxity followed by scarping of the tarsal conjunctiva of lateral tarsal strip. The expected amount of LTS can be assessed and fixating sutures is placed through the tarsal strip and the periosteum of lateral orbital wall by 5/0 prolene suture which is at least 2 mm superior to medial canthus. The periosteal bite should be confirmed by pulling the sutures and tied the suture; second suture is placed as in the same manner. Finally, the lateral canthus is reconstructed with 6/0 vicryl buried suture into gray line followed by closure of skin and orbicularis oculi muscle with 6/0 vicryl sutures accordingly. The procedure is demonstrated in [Figure 1], [Figure 2].
Results
We assessed the outcome of LTS procedure for 48 lower eyelids marginal malposition of 43 patients. 38(88.4%) cases were unilateral and 5(11.6%) cases were bilateral eyelid marginal malposition. Among the bilateral cases, 3(60%) were involutional entropion and 2(40%) were involutional ectropion. Group A included 24(50%) eyelids with involutional entropion of 21 patients, and group B included 24(50%) eyelids with involutional ectropion of 22 patients [[Table 1]]. This evaluated 31(72%) male and 12 female (28%). The mean age ± SD was 68.49± 9.97 years with the age range from a minimum of 54 years to a maximum of 90 years. Forty-five (93.7%) eyelids obtained satisfactory outcome after correction of involutional lower eyelid entropion and ectropion by the LTS procedure alone within one year followed up period. Three eyelids (6.3%) showed recurrences after 6 months of the LTS procedure. Among the recurrence cases, two (8.3%) were involutional ectropion (Group B) and another one (4.2%) was involutional entropion (Group A).
The success rate was 95.8%, and 91.7% of lower eyelids involutional entropion, and involutional ectropion respectively. The difference between the success and recurrence of involutional entropion and involutional ectropion was not statistically significant. Chi-square test was done and The p-value was >0.05. Overcorrection was assessed in 3 eyelids (8.3%) of involutional entropion which was resolved within 3 weeks of surgery. Mild ecchymosis was observed in 45 (93.7%) eyelids in early postoperative days, mild to moderate pain was presented in all (100%) cases up to 3 days of surgery, Feeling the discomfort in the lower eyelid (41 cases, 85.4%), and feeling of tightness at lateral canthus (95.8%). The feeling of tightness of the lower eyelid and tightness of lateral canthus were stabilized after 1 to 2 weeks of LTS procedure.
|
Parameters |
Group A |
Group B |
Results |
||
|
|
No. |
% |
No. |
% |
|
|
Patients: |
21 |
48.8 |
22 |
51.2 |
43 |
|
Eyelids |
24 |
50 |
24 |
50 |
48 |
|
Unilateral |
18 |
85.7 |
20 |
91 |
38 (88.3%) |
|
Bilateral |
03 |
14.3 |
02 |
09 |
05 (11.7%) |
|
Male |
15 |
71.4 |
16 |
72.7 |
31 (72%) 12 (28%) |
|
Female |
06 |
28.6 |
06 |
27.3 |
|
|
M:F |
2.5:1 |
2.6:1 |
2.6:1 |
||
|
Age Distribution: |
|
|
|
||
|
Mean Age ± SD (Year) |
66.67 ± 9.85 |
70.68 ± 9.52 |
68.49 ± 9.97 |
||
|
Median age |
63 |
67 |
66 |
||
|
Age Range |
54 y to 87 y |
59 y to 90 y |
54 y to 90 y |
||
|
95% CI |
62.18 to 71.15 |
66.46 to 74.90 |
65.42 to 71.56 |
||
|
Recurrence (eyelids) |
01 4.2 |
02 8.3 |
χ² value=0.356, df=1 p-value= >0.5ns |
||
|
Success (eyelids) |
23 95.8 |
22 91.7 |
Discussion
Involutional entropion and ectropion cause an imbalance forces on the lower eyelid and causes irritation to the globe and may cause corneal ulcer which leads to loss of vision.[4], [5] Surgical correction is the treatment of choice. There are various surgical options are described in the literature to correct involutional entropion and involutional ectropion. The Lateral tarsal procedure is a unique procedure by which both involutional entropion and ectropion can be corrected. Understanding eyelid anatomy and through knowledge of surgical procedure are essential for the correction of eyelid marginal malposition. Both entropion and ectropion are of different clinical entities but can present similar ocular symptoms. Lateral tarsal strip (LTS) technique is a simple and unique procedure to correct both ectropion and entropion of lower eyelid.[6], [7] The LTS procedures help in stabilization of the horizontal length of the lower eyelid and also correct the lateral canthal laxity. We studied 24 eyelids with involutional entropion of 21 cases (group A), and 24 eyelids with involutional ectropion of 22 cases (group B). Male (72%) is more prone to female (28%) for eyelid malposition in our study. The mean age is 66.67 year of group A, and 70.68 year of group B patients respectively. The satisfactory outcome of LTS procedure alone is evaluated in the 45(93.7%) eyelids in both groups of our study. The recurrence is noted in one eyelid (4.2%) of group A, and two eyelids (8.3%) of group B during the follow up period. LTS with infraciliary rotation appears to be a safe and effective technique to repair involutional eyelid entropion with a very high success rate (97.5%) and minimal recurrence rate (2.5%) in 39 eyelids. ocular irritation and discomfort are relieved in 97.7% cases and careful examination is required to ensure the cause of entropion prior to initiating surgical intervention.[8] 22.2% patients developed postoperative complications of LTS procedure.[7] The lagophthalmos, superficial punctate keratopathy (SPK) are evaluated preoperatively and all the symptoms are resolved postoperatively. Combined lateral tarsal strip with minimal tarsorrhaphy is an easy, safe, and most effective surgical technique for the management of the lower eyelid paralytic ectropion. It causes minimal aesthetic disfigurement and low morbidity during the long-term follow up.[9] López-García J.S et al. reported that recurrence is evaluated in 8 entropion eyelids (17.4%) and one ectropion eyelid (2.3%) of the 90 eyelids malposition which was corrected by the conventional LTS procedure in one group. The Recurrence is found in only 2 entropion eyelids (4%) in 94 eyelids malposition and repaired by a modified tarsal strip technique in another group. The horizontal laxity of the eyelid is improved in both groups after surgery. There were significant differences among the patients those who were treated with the modified technique (P=0.04). The modified suture placement of the LTS improved the stability of the lower eyelid and prevented recurrences after surgery. The modified LTS technique is helpful for the treatment of patients with entropion and ectropion.[10] The correction of ectropion by LTS with double sutures and conjunctival trimming showed improving the lower horizontal laxity than conventional LTS technique. LTS including double suture and conjunctival cuts showed a better ectropion correction with reducing grade and recurrences.[11] Jones retractor plication (JRP) alone in 61 patients and compared with JRP with a LTS in 57 patients for the corrected of involutional entropion was evaluated in a study and reported that JRP + LTS technique come with a higher success rate compared to JRP alone.[12] Minimal ecchymosis is observed in all cases of our study which was resolved within 2 weeks of surgery. All patients are felt mild postoperative pain up to 3 days of surgery. All the patients were happy and satisfied with the relief of epiphora, and foreign body sensation from their eyes. We performed a combined surgery (Dacryocystectomy with LTS) for the management of chronic dacryocystitis and involution entropion of the same eye. The combined surgeries (lacrimal drainage surgery with LTS) are effected techniques for the management of nasolacrimal duct obstruction and lower lid laxity. [13] LTS is helping to restore the normal lid function and gives a rapid rehabilitation and best aesthetic outcome.[14] Transverse everting sutures can be performed in combination with LTS for the better outcome for the correction of involutional entropion.[14], [15]
Conclusion
Lateral tarsal strip (LTS) procedure is easy, simple, and unique surgical technique to correct the lower eyelid malposition of different etiology and it can be performed with an additional technique to achieve the best surgical outcome.
Conflict of Interest
The authors declare no potential conflicts of interest.
Source of Funding
No funding was received for this study.
References
- KV, Ford R, Garrott H, Thaller V. Lateral tarsal strip versus Bick’s procedure in correction of eyelid malposition. Eye. 2018;32(6):1117-22. [Google Scholar] [Crossref]
- Collin J. A manual of systematic eyelid surgery. 3rd edn.. 2006. [Google Scholar]
- Jordan DR, Anderson RL. The lateral tarsal strip revisited. The enhanced tarsal strip. Arch Ophthalmol. 1989;107:604-6. [Google Scholar]
- Wright M, Bell D, Scott C, Leatherbarrow B. Everting suture correction of lower lid involutional entropion. Br J Ophthalmol. 1999;83(9):1060-3. [Google Scholar] [Crossref]
- Bosch WAvd, Leenders I, Mulder P. Topographic anatomy of the eyelids, and the effects of sex and age. Br J Ophthalmol. 1999;83(3):347-52. [Google Scholar] [Crossref]
- Fradinho N, Pereira A, Rasteiro D, Sousa J, Tojo N, Martins J. Lateral tarsal strip technique for lower lid ectropion and entropion. Int J Oral and Maxillofac Surg. 2013;42(10):1322-5. [Google Scholar] [Crossref]
- Al-Taher AAM, Awadeen AER. Lateral Tarsal Strip, Can It Be One Solution for All Types of Lower Eyelid Malposition?. Egypt J Hospital Med. 2019;75(5):2745-7. [Google Scholar]
- Rabinovich A, Allard F, Freitag S. Lower Eyelid Involutional Entropion Repair with Lateral Tarsal Strip and Infraciliary Rotation Sutures: Surgical Technique and Outcomes. Orbit. 2014;33(3):184-8. [Google Scholar] [Crossref]
- Kwon KY, Jang AY, Yoon JS. Long-term outcome of combined lateral tarsal strip with temporal permanent tarsorrhaphy for correction of paralytic ectropion caused by facial nerve palsy. J Craniofac Surg. 2015;26(5):409-12. [Google Scholar]
- López-García JS, García-Lozano I, Giménez-Vallejo C, Jiménez B, Sánchez A. Elosua de-Juan I. Modified lateral tarsal strip for involutional entropion and ectropion surgery. Graefe's Arch for. Clin and Exp Ophthalmol. 2017;255:619-25. [Google Scholar]
- Meduri A, Inferrera L, Oliverio G, Tumminello G, Rechichi M, Mazzotta C. The Use of a Double Suture and Conjunctival Cuts in the Lateral Tarsal Strip: A New Approach to Involutional Ectropion. J Craniofac Surg . 2018;29(8):2312-5. [Google Scholar] [Crossref]
- Ranno S, Sacchi M, Gilardi D, Lembo A, Nucci P. Retractor Plication versus Retractor Plication and Lateral Tarsal Strip for Eyelid Entropion Correction. Euro J Ophthalmol . 2014;24(2):141-6. [Google Scholar] [Crossref]
- Lee H, Hwang J, Kim JW, Park M, Baek S. The Effectiveness of Simultaneous Lateral Tarsal Strip With Endonasal Dacryocystorhinostomy for the Treatment of Nasolacrimal Duct Obstruction and Lower Lid Laxity. J Craniofac Surg. 2013;24(3):980-3. [Google Scholar] [Crossref]
- Olver J. Surgical tips on the lateral tarsal strip. Eye. 1998;12(6):1007-12. [Google Scholar] [Crossref]
- Barnes J, Bunce C, Olver JM. Simple Effective Surgery for Involutional Entropion Suitable for the General Ophthalmologist. Ophthalmol. 2006;113(1):92-6. [Google Scholar] [Crossref]