- Visibility 473 Views
- Downloads 73 Downloads
- Permissions
- DOI 10.18231/j.ijooo.2020.046
-
CrossMark

Abstract
Purpose: The aim of this study is to report the efficacy of topical Mitomycin-C (MMC) as adjunctive treatment following primary excision of ocular surface squamous neoplasia (OSSN).
Materials and Methods: After detailed evaluation, 25 eyes in 25 patients with localized primary OSSN were selected in a prospective, interventional study and subjected to primary excision followed by the application of topical 0.04% MMC as an adjunct and thereafter followed up over a 24 month period for signs of any tumor recurrence. Result: The 25 patients selected with primary OSSN had a mean age of 64(SD 13) with a range of 47-87 years. They underwent surgical excision followed by 3 cycles of freshly prepared 0.04% MMC with 2 weeks on and 2 weeks off for 12weeks.All patients were followed up thereafter at 1 week, 2 weeks, monthly for 6 months and every 3 months for the next 24 months. No tumor recurrence was observed in any of the cases.
Conclusion: Topical MMC has a definite role in preventing tumor recurrence when used as adjunctive treatment following primary surgical excision of OSSN.
Introduction
Ocular surface squamous neoplasia (OSSN) encompasses a spectrum of epithelial squamous malignancies, that range from mild to severe dysplasia to invasive squamous cell carcinoma.[1] The incidence of OSSN across the world has been reported to be 0.02-3.5 cases per 100,000, [2] with a greater frequency in regions near the equator. [3] OSSN generally presents in the late sixth to seventh decades of life, but has been seen to occur earlier in people who are immunocompromised. [4] Several risk factors have been implicated in causing OSSN which include UV light exposure, an immunocompromised state as in HIV and Human Papilloma Virus infection, [5] smoking, [6] advanced age and male gender. [7]
The mainstay of treatment of OSSN involves surgical excision. However, a high rate of recurrence has been observed following surgical excision alone. Therefore, several adjunctive therapies have been described, which have been found to be effective in preventing tumor recurrence. Herein, we undertook a study of 25 eyes in 25 patients with localized primary OSSN who were treated with surgical excision and topical Mitomycin -C(MMC) as an adjunct and have reported the recurrence rate after a follow -up period of 24 months.
Materials and Methods
After seeking ethical committee approval and written consent from the patients, the study was conducted in our institute. The study conducted was a hospital based, prospective interventional study that involved 25 eyes of 25 patients with localized OSSN who presented between January 2017 to January 2020.
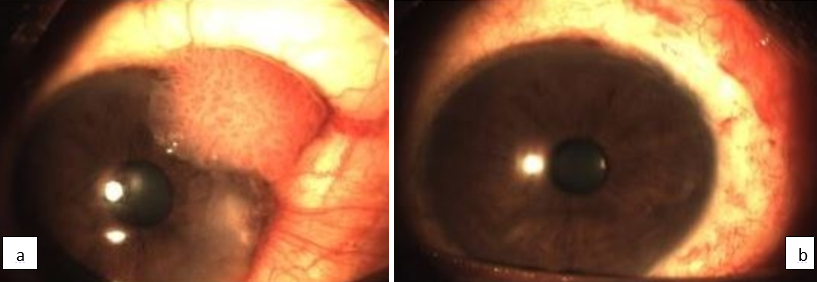
A detailed history including demographic details, duration of symptoms and risk factor exposure were recorded. A thorough clinical examination was conducted that included visual acuity assessment, a detailed anterior segment evaluation including the shape, size, mobility and extent of the lesion, any anterior chamber reaction, fluorescein staining under slit lamp biomicroscopy, fundus evaluation and lymphadenopathy. Inclusion criteria involved localized non-invasive OSSN (with associated corneal involvement as visualized on slit lamp evaluation and confirmed on histopathological examination. ([Figure 1]a). Patients with advanced disease were excluded from the study.
The protocol for management involved complete surgical excision of the lesion with a 2mm healthy rim and the excised tissue was sent for hisptopathological examination. The surgical excision was carried out by the same operating surgeon in all the cases. The ocular surface was left to heal or amniotic membrane transplantation done in case the defect created was more than 4mm in size. After the corneal epithelial surface healed completely, 0.04% solution of Mitomycin-C (MMC) was prepared by reconstituting a 2mg/ml MMC vial with 5ml of sterile distilled water. The solution was refrigerated after reconstitution. All patients received freshly prepared topical 0.04% MMC and were instructed to instill it four times a day as eye drops and continue for 3 cycles with 2 weeks on and 2 weeks off for 12weeks. The patients were followed up at 1 week, 2 weeks, monthly for 6 months and thereafter every 3 months for the next 24 months. At each visit a thorough slit lamp evaluation was performed along with fluorescein staining and routine examination for any corneal keratitis or erosions and to look for any tumor recurrence ([Figure 1] b). The effectiveness of MMC was assessed in the form of tumor recurrence. ([Table 1])
| Patient | Age at Dx | R/L eye | Location | Histopathology | Treatment | MMC S/E | No. of course | Recurrence |
| 1 | 56 | L | Nasal limbal | CIN I | E, 0.04%MMC | None | 3 | No |
| 2 | 75 | R | Nasal limbal | CINI | E, 0.04%MMC | Allergy | 2 | No |
| 3 | 57 | R | Temporal limbal | CIN II | E, 0.04%MMC | None | 3 | No |
| 4 | 86 | R | Temporal limbal | CIN III | E, 0.04%MMC | None | 3 | No |
| 5 | 52 | L | Nasal limbal | CIN I | E, 0.04%MMC | None | 3 | No |
| 6 | 57 | L | Limbal | CIN II | E, 0.04%MMC | None | 3 | No |
| 7 | 61 | R | Nasal limbal | CIN III | E, 0.04%MMC | None | 3 | No |
| 8 | 57 | L | Temporal limbal | CIN I | E, 0.04%MMC | Allergy | 2 | No |
| 9 | 62 | L | Nasal limbal | CIN I | E, 0.04%MMC | None | 3 | No |
| 10 | 53 | L | Nasal limbal | CIN III | E, 0.04%MMC | Allergy | 2 | No |
| 11 | 50 | L | Temporal limbal | CIN II | E, 0.04%MMC | None | 3 | No |
| 12 | 69 | R | Nasal limbal | CIN III | E, 0.04%MMC | None | 3 | No |
| 13 | 53 | L | Temporal limbal | CIN II | E, 0.04%MMC | None | 3 | No |
| 14 | 70 | R | Temporal limbal | CIN I | E, 0.04%MMC | None | 3 | No |
| 15 | 63 | R | Nasal limbal | CIN II | E, 0.04%MMC | None | 3 | No |
| 16 | 41 | R | Temporal limbal | CIN III | E, 0.04%MMC | None | 3 | No |
| 17 | 75 | L | Nasal limbal | CIN II | E, 0.04%MMC | None | 3 | No |
| 18 | 61 | L | Temporal limbal | CIN III | E, 0.04%MMC | None | 3 | No |
| 19 | 57 | R | Nasal limbal | CIN III | E, 0.04%MMC | None | 3 | No |
| 20 | 76 | L | Temporal limbal | CIN I | E, 0.04%MMC | Allergy | 2 | No |
| 21 | 82 | R | Nasal limbal | CIN II | E, 0.04%MMC | None | 3 | No |
| 22 | 49 | L | Temporal limbal | CIN I | E, 0.04%MMC | Allergy | 2 | No |
| 23 | 47 | R | Nasal limbal | CIN I | E, 0.04%MMC | None | 3 | No |
| 24 | 73 | L | Temporal limbal | CIN III | E, 0.04%MMC | None | 3 | No |
| 25 | 67 | R | Limbal | CIN II | E, 0.04%MMC | None | 3 | No |
| CIN=Conjunctival intraepithelial neoplasia, E=excision, MMC=Mitomycin-C, S/E=side effects |
Results
Of the 25 patients, there were 7 females and 18 males, with 25 primary OSSN as depicted in [Table 1], clearly indicating a male preponderance. The mean age was 64 (SD 13) with a range of 47-87 years. Of the 25 patients who underwent surgical excision, 20 patients received 3 cycles of freshly prepared 0.04% MMC with 2 weeks on and 2 weeks off for 12 weeks. 5 patients (20%) developed an allergic response to MMC in the form of mild redness and itching, because of which they received only 2 courses of 0.04% MMC. The symptoms of MMC allergy resolved completely after discontinuation of therapy. All patients were followed up thereafter at 1 week, 2 weeks, monthly for 6 months and every 3 months for the next 24 months and underwent a thorough evaluation for tumor recurrence at each visit. However, there was no tumor recurrence in any of the cases.
Discussion
Our study involved 25 eyes of 25 patients with localized OSSN who presented between January 2017 to January 2020 for which they underwent surgical excision followed by 0.04% MMC.
The mean age at presentation was 64 with a range of 47-87 years.[8] The patients did not report any recurrence of tumor after a follow-up period of 24 months, thereby indicating a successful outcome.
OSSN has been reported to be the most common malignancy of the conjunctiva and cornea. [1] Primary surgical excision has been the mainstay of treatment of OSSN. Surgical excision facilitates debulking of the tumor and allows an immediate histopathological diagnosis. Surgical excision when used only has a major disadvantage in the form of a high recurrence rate ranging from 15% to 52%. [9] Therefore several adjunctive treatments have come up which help in decreasing tumor recurrence .Chemotherapeutic agent in the form of Mitomycin-C (MMC) is one such adjunctive therapy. MMC is an alkylating agent which is a DNA synthesis inhibitor and causes cell necrosis and apoptosis. [10] Several studies have reported the use of MMC for both primary and recurrent cases of OSSN with successful outcome. [11], [12], [13], [14], [15], [16], [17]
MMC has another advantage that it allows treatment of the entire ocular surface including the conjunctival fornices and thus can destroy subclinical disease and prevent the formation of new tumors elsewhere on the ocular surface. Complications with MMC are common as is evident in our study wherein 5 out of 25 patients (20%) reported an allergic response to MMC in the form of mild redness and itching, which resolved after discontinuing treatment. However, none of our patients reported any other serious complications like uveitis, glaucoma, cataract and scleral ulceration [18], as we had ensured complete epithelial healing and the week on-off regimen of MMC application .
Conclusion
To conclude, our study demonstrates that using 0.04% MMC after surgical excision of OSSN leads to a decrease in the recurrence rate and is therefore an effective adjunctive therapy in cases of primary ocular surface squamous neoplasia.
Acknowledgements
None.
Source of Funding
None.
Conflict of Interest
None
References
- Lee GA, Hirst LW. Ocular surface squamous neoplasia. Survey Ophthalmol. 1995;39(6):429-50. [Google Scholar]
- Yang J, Foster CS. Squamous Cell Carcinoma of the Conjunctiva. Int Ophthalmol Clin. 1997;37(4):73-85. [Google Scholar]
- Gichuhi S, Sagoo MS, Weiss HA, Burton MJ. Epidemiology of ocular surface squamous neoplasia in Africa. Trop Med Int Health. 2013;18(12):1424-43. [Google Scholar]
- Porges Y, Groisman GM. Prevalence of HIV With Conjunctival Squamous Cell Neoplasia in an African Provincial Hospital. Cornea. 2003;22(1):1-4. [Google Scholar]
- Gichuhi S, Ohnuma S, Sagoo MS, Burton MJ. Pathophysiology of ocular surface squamous neoplasia. Exp Eye Res. 2014;129:172-82. [Google Scholar]
- Napora C, Cohen EJ, Genvert GI, Presson AC, Arentsen JJ, Eagle RC. Factors associated with conjunctival intraepithelial neoplasia: A case control study. Ophthalmic Surg. 1990;21:27-30. [Google Scholar]
- Gichuhi S, Macharia E, Kabiru J, Zindamoyen AM, Rono H, Ollando E. Clinical Presentation of Ocular Surface Squamous Neoplasia in Kenya. JAMA Ophthalmol. 2015;133(11):1305-13. [Google Scholar]
- Shields CL, Shields JA. Tumors of the conjunctiva and cornea. Survey Ophthalmol. 2004;49(1):3-24. [Google Scholar]
- Kaines A, Davis G, Selva D, Leibovitch I, Dodd T, Malhotra R. Conjunctival Squamous Cell Carcinoma With Perineural Invasion Resulting in Death. Ophthalmic Surg, Lasers Imaging Retina. 2005;36(3):249-51. [Google Scholar]
- Sudesh S, Rapuano CJ, Cohen EJ, Eagle RC, Laibson PR. Surgical Management of Ocular Surface Squamous Neoplasms. Cornea. 2000;19(3):278-83. [Google Scholar]
- McKelvie PA. Impression cytology following mitomycin C therapy for ocular surface squamous neoplasia. Br J Ophthalmol. 2001;85(9):1115-9. [Google Scholar]
- Frucht-Pery J, Rozenman Y. Mitomycin C Therapy for Corneal Intraepithelial Neoplasia. Am J Ophthalmol. 1994;117(2):164-8. [Google Scholar]
- Frucht-Pery J, Sugar J, Baum J, Sutphin JE, Pe’er J, Savir H. Mitomycin C Treatment for Conjunctival—Corneal Intraepithelial Neoplasia. Ophthalmol. 1997;104(12):2085-93. [Google Scholar]
- HEG, TMA. Mitomycin C Treatment of Conjunctival Intraepithelial Neoplasia. Am J Ophthalmol. 1997;124(3):381-2. [Google Scholar]
- Heigle TJ, Stulting RD, Palay DA. Treatment of recurrent epithelial neoplasia with topical mitomycin C. Am J Ophthalmol. 1997;124:397-9. [Google Scholar]
- Kemp EG. Preoperative topical and intraoperative local mitomycin C adjuvant therapy in the management of ocular surface neoplasias. Br J Ophthalmol. 2002;86(1):31-4. [Google Scholar]
- Ballalai PL, Erwenne CM, Martins MC, Lowen MS, Barros JN. Long-Term Results of Topical Mitomycin C 0.02% for Primary and Recurrent Conjunctival-Corneal Intraepithelial Neoplasia. Ophthalmic Plast Reconstr Surg. 2009;25(4):296-9. [Google Scholar]
- Daniell M, Maini R, Tole D. Use of mitomycin C in the treatment of corneal conjunctival intraepithelial neoplasia. Clin Exp Ophthalmol. 2002;30(2):94-8. [Google Scholar]